SIS is a simple real time ultrasound procedure. Few millilitre of sterile saline are instilled slowly into the uterine cavity to separate the anterior and posterior uterine walls. It is hypoechoic and would act as a negative contrast medium which would help in revealing any endometrial or subendometrial pathology as well as delineating the shape of the cavity. It is an easy procedure to perform with minimal intrusion and discomfort. Nevertheless, patients are advised to take an over the counter analgesic one hour before the procedure. Any clear fluid could be used instead of saline and a local anaesthetic would be an excellent choice if either an endometrial biopsy or polypectomy were planned, as it would help in reducing pain. To have stable filling of the uterine cavity and reduce outflow through the fallopian tubes, hydroxyethylcellulose gel containing a local anaesthetic and an antiseptic has been used by Exalto et al [2007] which resulted in high quality ultrasonic visualisation of the cavity. The author of this manuscript had similar experience using instillagel in patients with very low pain threshold with excellent effect as well. It is a sterile lubricant, local anaesthetic and disinfectant for mucosa sold in disposable syringes (CliniMed, Cavell House, Knaves Beech Way, High Wycombe, Buck HP10 9QY).
The procedure should be done immediatelyafter menstruation when only the basal endometrial layer would be seen with a total measurement of 4 mm. Postmenopausal women on cyclic HRT should have SIS immediately after finishing a withdrawal bleeding. However, those on combined HRT could have it at any time as the endometrium thickness is not significantly affected by the combined HRT. This would avoid any artefacts caused by hormone induced endometrial changes. Accordingly, any higher measurements could be caused by polyps, intracavitary fibroids or incomplete endometrial shedding possibly due to endometrial hyperplasia. A high percentage of false positive findings would be seen if the procedure is done later on during the cycle or the catheter is pushed into the uterine cavity causing detachment of endometrial fragments. A figure of 27% of false positive results has been quoted before when the procedure was done after the 10th day ofthe cycle[Wolman et al 1999].
Technique
To gain patients confidence and reduce apprehension and pain thorough explanation should be given before starting the procedure. The bladder should be empty and the patient should be well covered in the lithotomy position. Each step should be explained to the patient beforehand and a simple running commentary should be given. Warm speculum and antiseptic fluid should be used.
After cleaning the vulva, vagina and cervix with an antiseptic, a soft thin catheter is introduced into the cervical canal and not into the uterine cavity itself. This would reduce discomfort and endometrial detachment which could result in a high false positive diagnosis of polyps. A Goldstein catheter is a good option as it is only 1.8 mm in diameter and its white acorn is applied to the external cervical os to reduce back flow leaking of the fluid. The catheter could be introduced through the side of the bivalve speculum and not down the channel. This would allow easy removal of the speculum without dislodging the catheter. Few millilitres of sterile saline are instilled slowly [to avoid pain] to distend the uterine cavity separating the front and back walls. The fluid will act as an echo-free area to delineate any endometrial pathology. This would allow an exact measurement of the endometrial thickness and would show any polyp, fibroid or synechiae missed during basic scanning. To minimise air artifacts which could interfere with proper visualisation of the cavity the catheter should be primed with saline before insertion into the cervical canal. Using ballooned catheters into the uterine cavity would interfere with complete visualisation and could lead to a high level of false negative findings. Such catheters should be used only in cases with patulous cervical canal, for examination of tubal patency and when high pressure is needed in cases with synechiae and large fibroids. The whole procedure should be videotaped to keep a record and allow further examinations in the future.
The uterus should be scanned initially in the longitudinal plane from one side to the other [from one conua to the other conrua]. The probe is then rotated 900 to scan the uterus in the axial plane from the fundus to the cervical canal. Usually few millilitres of fluid are needed to visualise the uterine cavity and unlike hysteroscopy complete distension of the cavity is not necessary. At the end of the procedure the catheter should be removed gently and the patient allowed to lie down for few minutes if she so wished. She should also be warned that she might have some blood loss for a short while after the procedure. We usually give a 5-day course of 100 mg doxycycline but in case of known allergy metronidazole is prescribed instead.
Please click on the following link to see how saline infusion showed a large fibroid did not affect the cavity in a patient with abnormal uterine bleeding:
SIS could be helpful in establishing a diagnosis in the following situations:
Abnormal uterine bleeding which is the most common indication
Abnormally thick endometrium echoes
Irregular or indefinite endometrial line
Indiscriminate intrauterine pathology
Suspected intrauterine adhesions in cases of amenorrhoea or hypomenorrhoea
Infertility investigations especially in cases with repeated miscarriages.
For follow up after hysteroscopic surgery especially after myomectomy and incision of a septum
It is important to remember that subendometrial pathology including adenomyosis, submucosal fibroids and subendometrial cysts could all show as thick endometrium during basic transvaginal scan examination.
Practical implications of the test
A thin endometrium [< 5mm] with an intact cavity would exclude the possibility of any endometrial pathology and the need for further invasive investigations. Each endometrial wall should be measured separately and the total measurement should not include the fluid in the cavity.
A universally thick endometrium would be well represented by an office endometrial biopsy.
A focal abnormal area would indicate a hysteroscopically targeted biopsy. Small focal lesions off the midline may be missed with an office biopsy which samples less than 5% of the cavity [Rodriquez G C et al, 1993, Am J Obstet Gynecol, 168: 55-59]
With such a simple procedure many women would avoid unnecessary invasive operations and the need for general anaesthesia. In our unit saline infusion sonohysterography has replaced diagnostic hysteroscopy as the second line of investigations for abnormal uterine bleeding. This is especially so since previous reports showed that a high percentage of submucosal fibroids could be missed with hysteroscopy which is only resorted to for operative purposes .
SIS revelations
A normal cavity appears as an anechoic space surrounded by symmetric endometrium on all sides.
Focal lesions are easier to see because each single layer of the endometrium is visible separately with saline acting as a background contrast medium.
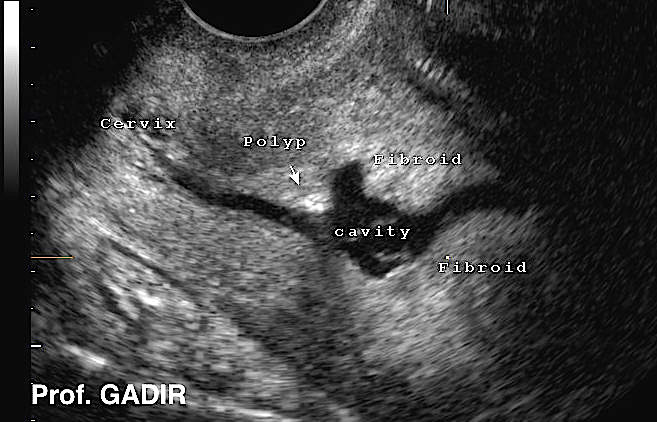
Polyps appear as echogenic structures surrounded by the anechoic fluid. The stalk might be evident at one side.
Submucous fibroids push into the cavity with normal overlying endometrium. They may be ehcogenic or relatively echo poor lesions with broad base continuous with the myometrium. They may as well cause shadowing.
Intrauterine adhesions may appear as bright bands across the cavity but as well they could prevent uterine cavity dilatation with saline, depending on the severity of the condition and location of the adhesions.
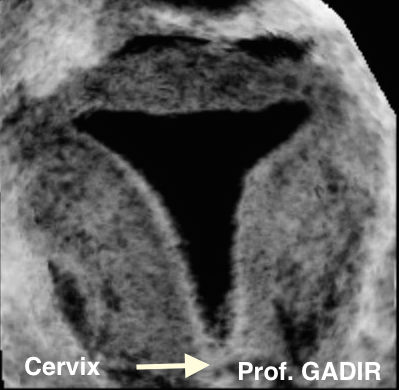
2D sagittal and 3D rendered images of a normal uterus after SIS. The 3D image shows a normal triangular cavity which is an important finding especially during investigation of recurrent miscarriages.
The first ultrasound image above shows thick uniform endometrium during saline infusion hysterography. In such cases an office biopsy will be representative of the whole endometrium. On the other hand, cases with focal endometrial lesions as shown by the second image above, should be investigated with hysteroscopy.
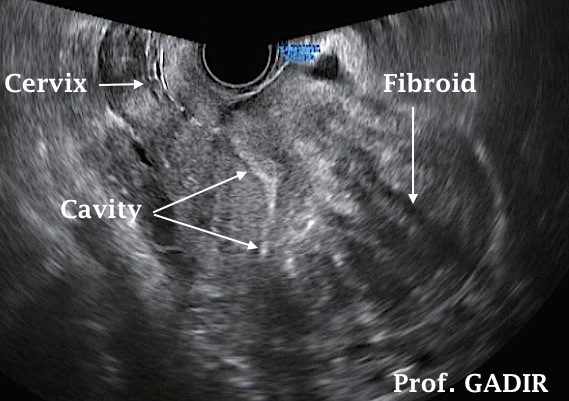
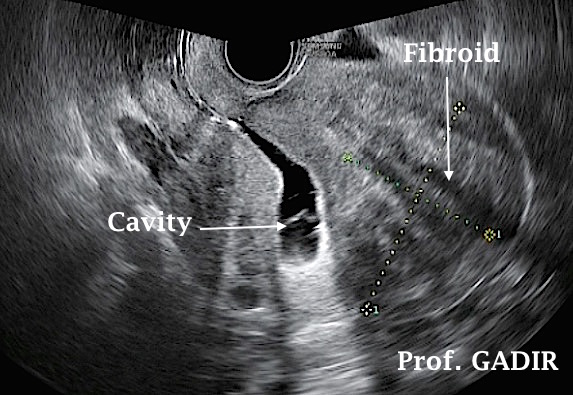
The first image above shows a sagittal view of a uterus with a large anterior uterine wall fibroid. The cavity was not clear in its upper part, and in its relationship to the fibroid.
The second image shows the same uterus, after saline infusion with an intact uterine cavity, not affected by the anterior wall fibroid. The endometrial line neighbouring the fibroid is very clear.
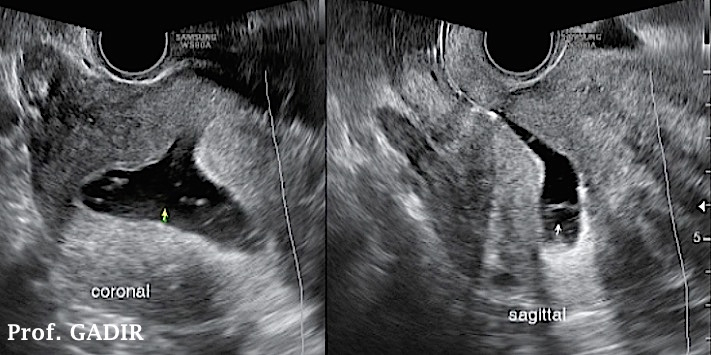
The third double image shows axial and sagittal views of the same uterus, after saline infusion, confirming a normal cavity in both planes.
The value of saline infusion in exploring the integrity is best shown by these three images.
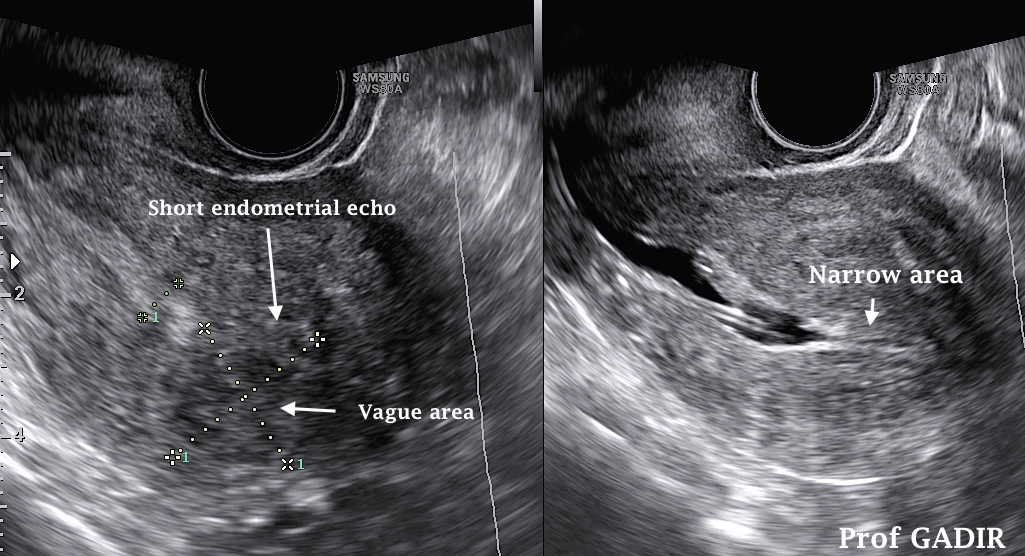
The neighbouring split image shows:
The left hand side image shows a short bright
endometrial stripe reaching half the way up to
the fundus, with a vague area on top of it.
The second saline hysterography image shows
an irregular lower cavity and a narrow upper
part of the cavity which did not dilate with
saline due to adhesions, represented by the
vague area seen in the left hand side image
Complications
SIS has minimal side effects in a well selected population of patients. Discomfort is the most common one though some patients might feel more cramps similar to period pains. Very rarely vasovagal reactions might occur even after the end of the procedure. These are mere nuisance in young women but could cause hypotension in older patients with atherosclerosis. Genle handling and prompt cessation of the procedure in response to patients' discomfort would reduce these risks. Infection is another risk but is rarely seen if aseptic techniques are used and the patients had no active or recent history of PID. We use routine antibiotics cover as mentioned before in all cases.
3D Ultrasound SIS
Volume acquisition of the uterus during 3D ultrasound examination while injecting saline allows archiving of a complete set of data to be examined in more detail and in different planes. It could also lead to a shorter and less manipulative procedure with smaller amount of saline injected, all contributing to less patients discomfort.
Though different studies showed 2D SIS to be equally diagnostic as 3D SIS, using the multiplanar technique after volume acquisition allows better identification of the exact nature and site of the intracavitary pathology which helps the treating physician planning his or her management.
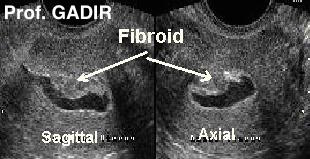
These 4 images show the following:
2D sagittal image of the uterus showing an echogenic abnormal area in the middle of the cavity. It does not show the exact nature of the pathology and how much of it is intracavitary.
The second image shows 2D sagittal and axial images of same uterus after instillation of saline.
The third image shows a 3D rendered coronal view of the same uterus after instillation of saline showing a submucous fibroid on the right side of the cavity. As well it delineates how much of the fibroid lies within the muscle or the uterine cavity. It was grade 0 in this case. This is an important piece of information prior to hysteroscopic excision.
The last image shows the same fibroid being removed during hysteroscopic examination.
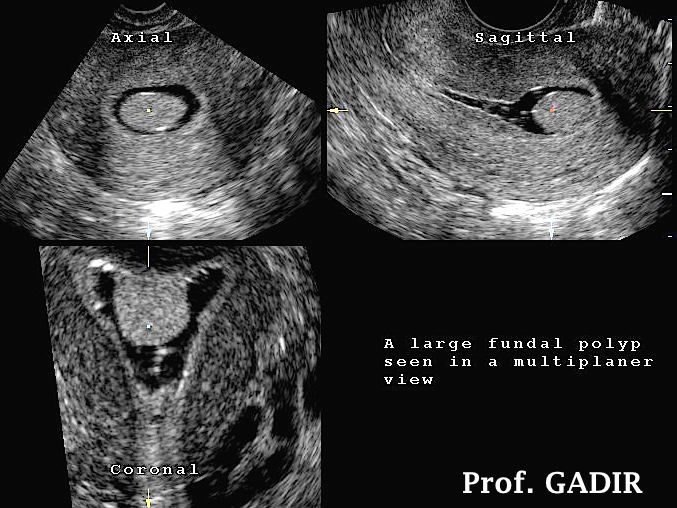
The neighbouring 3D multiplanar image shows an endometrial polyp in axial, sagittal and coronal sections. It gives a very clear visual picture about where exactly the polyp is located
Tamoxifen effect
It is a known fact that tamoxifen could cause endometrial hyperplasia, endometrial polyps or even cancer. Nevertheless regular screening of patients recieving this medication has not been recommended. However patients on tamoxifen who develp abnormal uterine bleeding should have thorough transvaginal scan examination to exclude such possibility. It is important to note that many of these patients might show subendometrial cysts in the junctions zone which could give a confusing pictre if saline infusion sonohysterography is not performed.
The 2D image shown above demonstrates an abnormal endometrium after exposure to tamoxifen for breast cancer. The second coronal 3D view shows the same uterus after saline infusion demonstrating subendometrial cysts [marked 1 and 2] with normal endometrium otherwise. These cysts resolved after stopping tamoxifen and using femara instead.