Endometrial polyps are localised overgrowth of the basal stroma with central blood vessels covered by surface endometrium mostly rising from the fundal area. Recent reports suggested clonal rearrangement of stromal chromosome 6p21 as the initial step triggering the development of polyps.
They could be seen in 10-15% of all women and could be associated with endometrial hyperplasia. They are rarely seen during teenage years. Their incidence increases with age to peak between 40 - 50 years before gradually declining after the menopause.
Polyps may be single or multiple, small or large, sessile or pedunculated, symptomatic or asymptomatic. In approximately 20% of cases they are multiple and in less than 1% are associated with malignancy. So polyps are typically single, small, asymptomatic and benign. However, the rate of malignancy depends on age, as well. Occasionally they cause:
postcoital bleeding
intermenstrual bleeding
heavy menstruation
vaginal discharge
postmenopausal bleeding especially in women on HRT.
This list shows that abnormal bleeding episodes to be the most important presenting problem related to endometrial polyps. In fact a previous study showed that 25% of all abnormal pre-and-postmenopausal bleeding to be caused by endometrial polyps. Accordingly polyps should be included in the provisional diagnosis of such cases and appropriate means taken to exclude them.
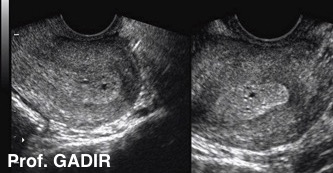
Ultrasonically a polyp could be seen as an echogenic mass splitting the central echo of a midcycle trilaminar endometrium. Otherwise they are best delineated with some fluid instilled into the cavity. On the other hand a fibroid disturbing the uterine cavity would be seen pushing the midline endometrium echo to one side rather than splitting it. Occasionally reversing colours could make a pathology more prominent as shown by the polyp below.
The first ultrasound image shows a sagittal view of a uterus with an echogenic polyp splitting the central endometrial echo, which is a characteristic of polyps.
The second image shows a similar view of a uterus with an intracavitay fibroid pushing the central endometrial echo to one side rather than splitting it.
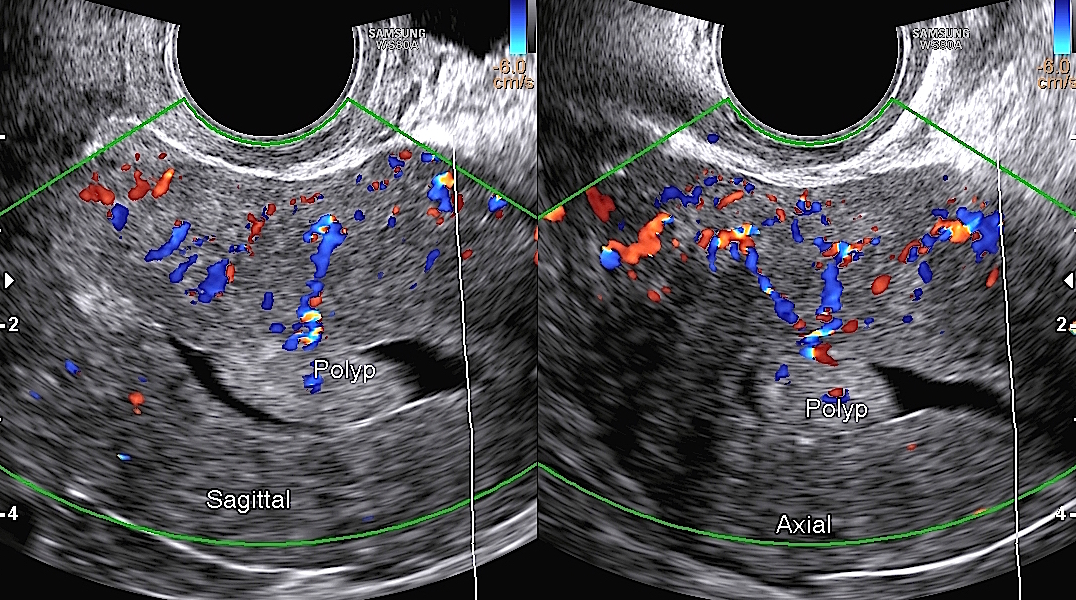
However, ultrasonic examination may fail to reveal endometrial polyps as they are usually echogenic and merge with the background echogenicity of the endometrium. Sometimes they show few anechoic areas due to entrapped mucous. Each polyp has central blood vessels which may be seen with colour Doppler mapping, as shown below.
The first double image above shows sagittal and axial views of a uterus with thick echogenic endometrium, showing sonolucent small areas. It was initially thought to be hyperplastic in nature.
The second 3D image of the same uterus showed instead multiple fundal polyps.
The third image demonstrated how saline infusion sonohysterography could also be useful. It revealed multiple posterior wall polyps, in a different patient who had a similarly thick and echogenic endometrium.
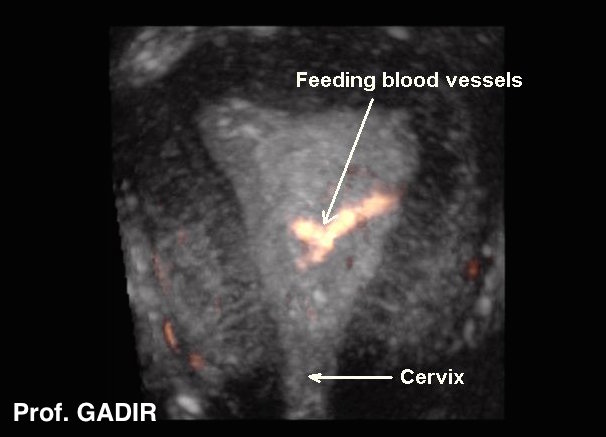
It is important to mention that liability of polyps to bleed follows their peculiar structure. Each polyp has a central feeding vessel, soft stroma and back to back glandularity.
The first image below shows a feeding vessel passing into an endometrial polyp, in sagittal and axial views. This is also a characteristic of polyps, which should be checked with colour Doppler, when available.
The second 3D image gives abetter picture of a large vessel passing into a polyp.
Once a diagnosis is established, a polyp should be removed using a resectoscope, especially if it has a broad base. The Author prefers this method, rather than using a hysteroscopic forceps, to to twist and avulse the polyp, which may leave some piece behind. The best time for carrying hysteroscopy is just after finishing menstruation. This will exclude the risk of missing a polyp within a thick endometrium, as expected later on during the cycle.
Blind D&C is no longer a valid operative option to remove polyps. A polyp may be pushed in front or sideway by the curette, missing it altogether. The removed polyp should be examined histologically to exclude any malignant changes.
The issue relating endometrial polyps to infertility or repeated miscarriages is a sticky one. Small polyps are not expected to have such an effect. However larger ones occupying a significant part of the cavity or obstructing tubal ostia, and symptomatic ones should be removed. This is especially so if no other cause has been demonstrated during other investigations. We also remove any polyp before starting assisted reproductive treatment.
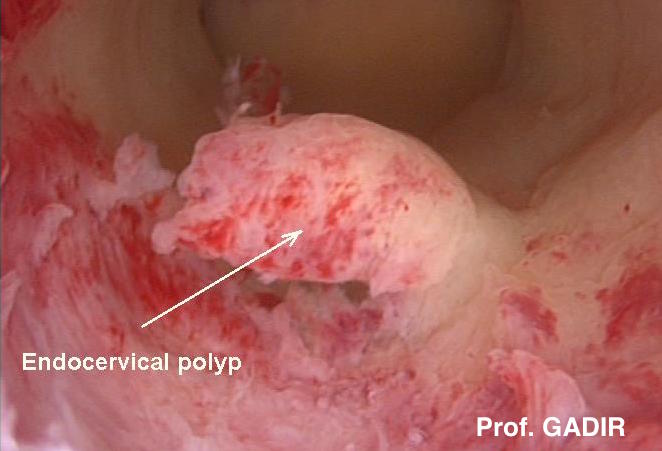
Endocervical polyps
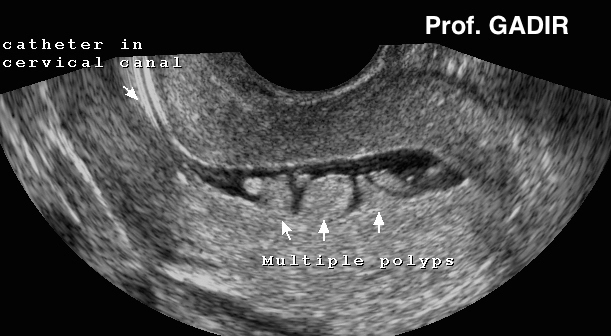
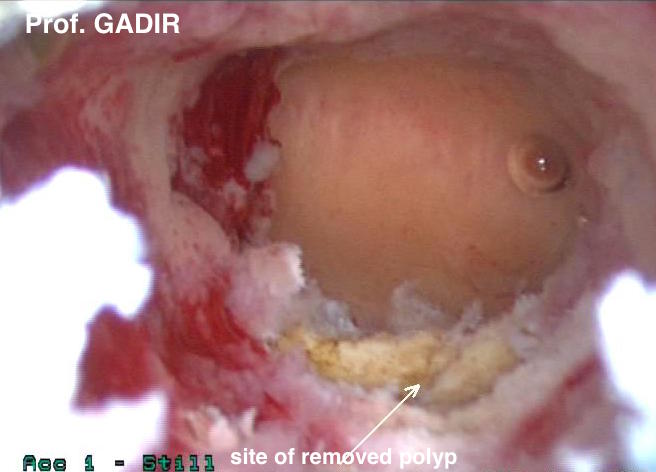
Occasionally, deep endocervical polyps may be missed during ultrasound scanning and hysteroscopy, if special care is not taken to examine the cervical canal. More often, the presence of mucous in the endocervical canal facilitates making such a diagnosis. Accordingly, ultrasound examination after exogenous oestrogen medication, or at ovulation time may facilitate such a diagnosis. The first ultrasound image shown below belongs to one patient who had many investigations for excessive vaginal discharge and intermenstrual bleeding before the diagnosis could be made with the help of mucous in the endocervical canal. The neighbouring two hysteroscopy images show the same polyp, and its site after being removed respectively
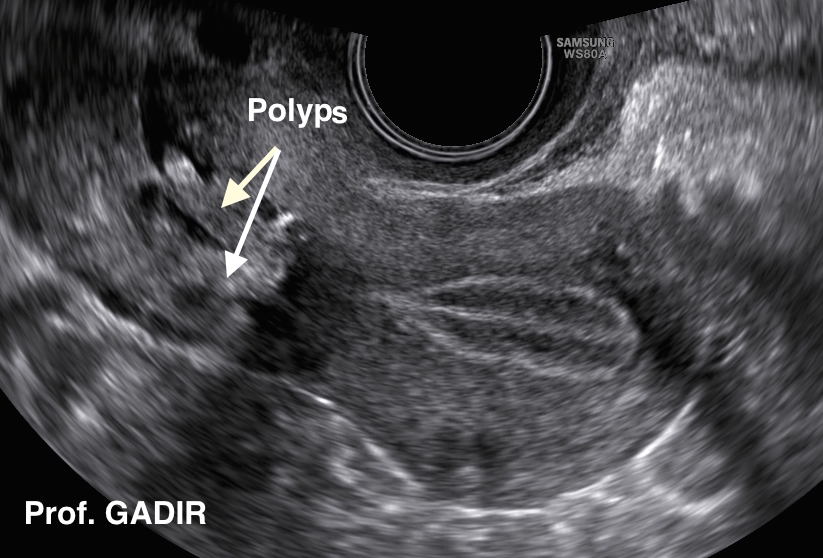
Sometimes it may be very difficult to diagnose endocervical polyps if more than one are cramping the limited endocervical canal space, even with he help of mucous in the cervical canal, as shown by the neighbouring image . It shows two polyps rising from the top part of the endocervical canal. The main complaint of this patient was copious mucoid vaginal discharge, which showed no pathogens on repeated high vaginal and endocervical swabs.