Gynaecological ultrasonography has become an integral part of the clinical examination. It is best done by the attending trained Gynaecologist to extend his or her clinical judgement. This is especially so in acute situations and in the areas of pelvic pain, abnormal uterine bleeding, early pregnancy monitoring and fertility investigations. Currently transvaginal scanning has taken over as the standard technique for pelvic examination. Both mechanical and electronic probes with offset or non-offset sound emission patterns could be used for transvaginal gynaecological scanning. For beginners the main difficulty is to convert from abdominal to transvaginal scan orientation. During transabdominal scanning both the monitor and the scanning plane are along the vertical axis. However this relationship is not true during transvaginal scanning as the probe and the monitor are in different planes. To have similar orientation to transabdominal scanning the monitor should be facing the roof during transvaginal scan examinations which is not the case in any of the ultrasound machines so far available.
Translabial scanning
Technique
When indicated, translabial scanning can be done to examine the rectum, anal sphincter and surrounding muscles. The probe should be kept in a vertical plane parallel to the two labia majora to examine the rectum, in its longitudinal axis. The probe can the be moved gently sideways to have an oblique view of the anal canal, and rectum. To view the circular anal orifice and surrounding muscles, the probe should be rotated 90 degrees, and move up and down to get the best image.
Perineal scanning is a neglected part of the gynaecological examination by most ultrasonographers. The following images shows the importance of such practice, especially in patient who present with vague vulval pain and superficial dyspareunia
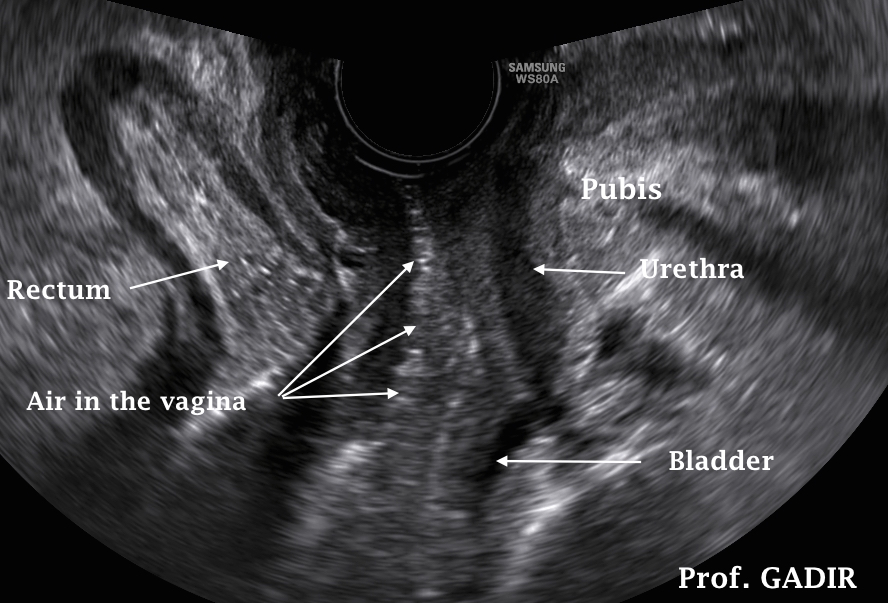
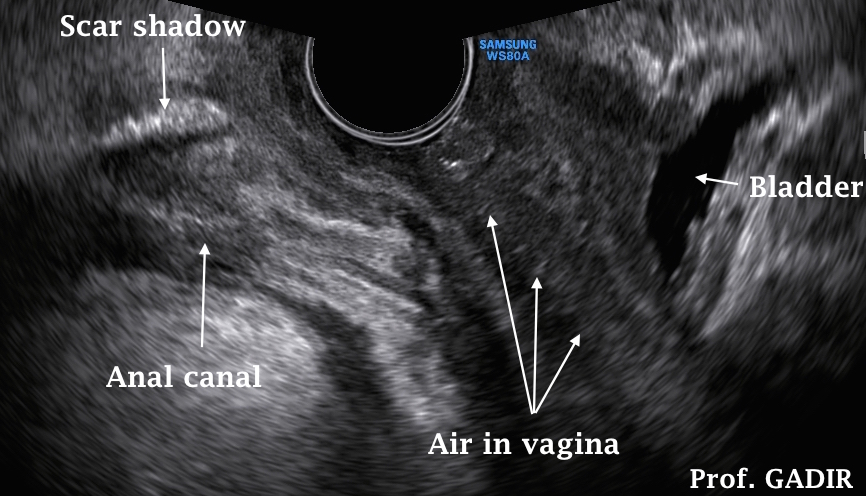
With modern machines and wide angle vaginal probes, a broader view of
the lower pelvis is possible. The neighbouring image shows a normal anal
canal and rectal ampulla. The bladder and urethra are also visible. The
vagina is marked by bright air specs in its lumen. Presence of air in the
vaginal lumen is important for proper identification of the exact location of
the vagina. This will facilitate the exact location of any pelvic pathology in
relation to the rectum, vagina and bladder, as will be demonstrated below.
Air may beintroduced into the vagina during speculum examination, or by
introducing the probe for some distance into the vagina and withdrawing it,
before starting the proper examination.
This double image shows a normal rectum in its sagittal section in the left
side image. The right side image shows a cross section of the lower part of
the anal canal. The anal sphincter is intact as well as the surrounding
muscles. This cross-section is important to examine the internal and
external anal sphincter muscles as well as the puborectalis muscle.
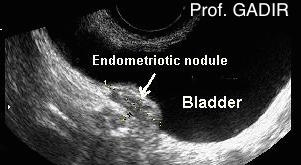
A slightly oblique Longitudinal view of the anal canal and rectum up to
therectal ampulla showing a circular mass on the front wall of the rectum.
This proved to be endometriotic nodule. The patient presented with
dyspareunia, as well as tenismus and diarrhoea, mainly during
menstruation
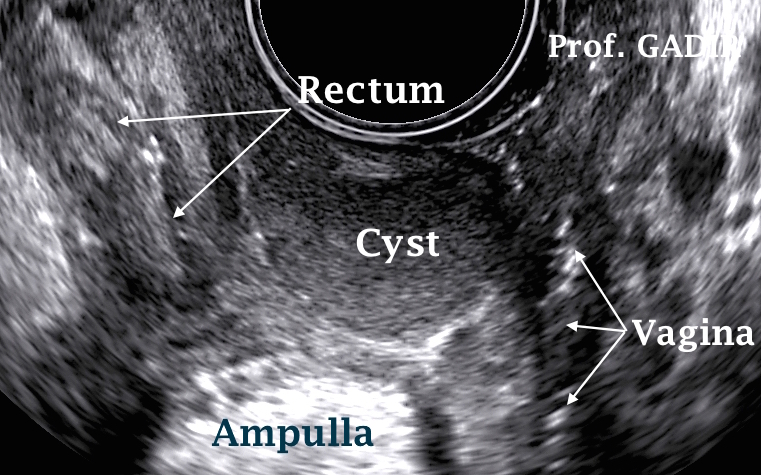
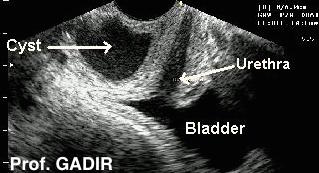
The neighbouring image shows a cystic area in between the vagina
anteriorly, the rectum posteriorly and and the rectal ampulla superiorly.
The importance of air in the vagina is well demonstrated in this image as
a good land mark to help in locating the exact position of the cyst. This
patient presented with superficial dyspareunia and vague perineal
discomfort while sitting down.
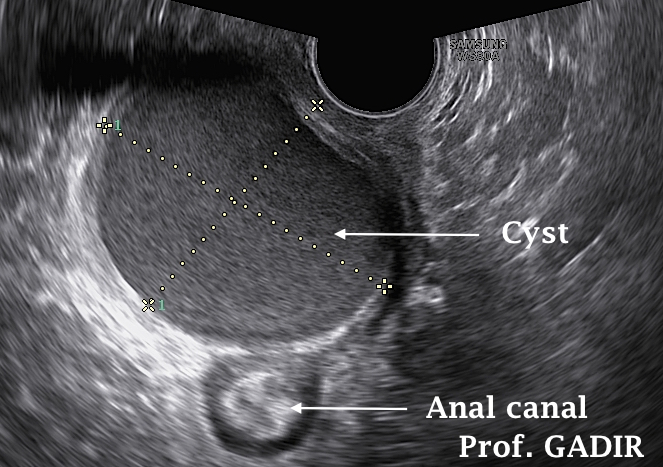
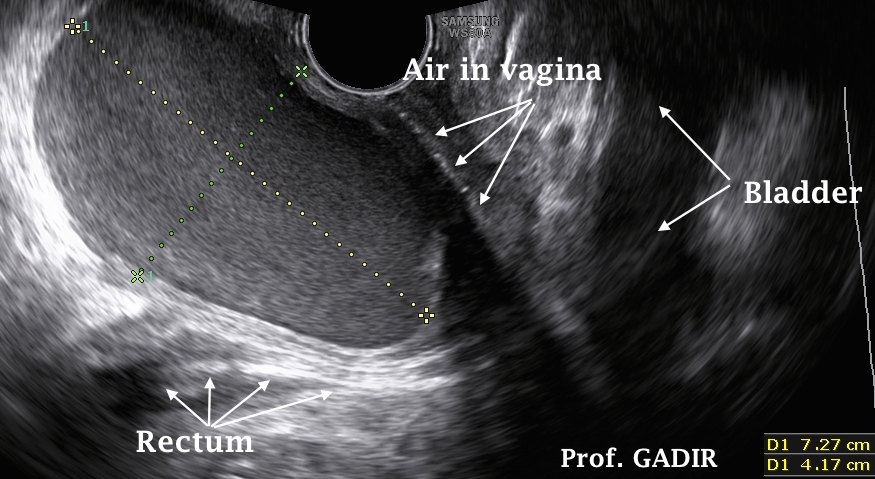
The two images shown below belong to one patient who presented with superficial dyspareunia and difficultly in opening her bowels. Superficial inspection of the vulva showed a vertical scar along the forchette, indicating previous surgery. The introitus admitted only one finger, while the patient felt intense pain. Using an endo-vaginal probe showed a large cystic mass between the anterior wall of the rectum and posterior vaginal wall, extending from just above the introitus to half way up the vaginal length. The left side image represents an axial view of the cyst anterior to the anal orifice, while the second image shows a longitudinal view of the cyst with the collapsed rectum underneath it, and the bladder pushed anteriorly. This cyst measured 7.2 x 5.4 x 4.1 cm.
Other than for vulval pain and superficial dyspareunia, perineal scanning is also important in women presenting with incontinence following surgery. Clinical examination may reveal some clues, but does not usually reveal the whole extent of the scar tissue or muscular deficiency involved. The following first two images belong to a woman who presented with difficulty in controlling her bowel motions and passing wind, beside having superficial dyspareunia following vaginal tightening after childbirth.
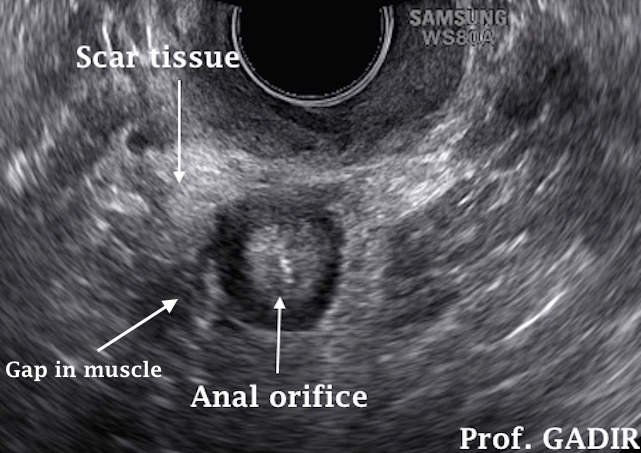
The first image below is an oblique view of the anal canal and rectum. There is a bright shadow on the anterior wall of the anal canal just to the right of the midline. This small area could have easily been ignored as an artefact.
The second image is a transverse view showing the anal orifice. There is a broad area of scarred tissue anterior to it. This scar tissue is more exaggerated to the right side with a thick irregular echogenic area. Despite the intense scarring, there is a gap in the anal sphincter muscle as 8 o'clock.
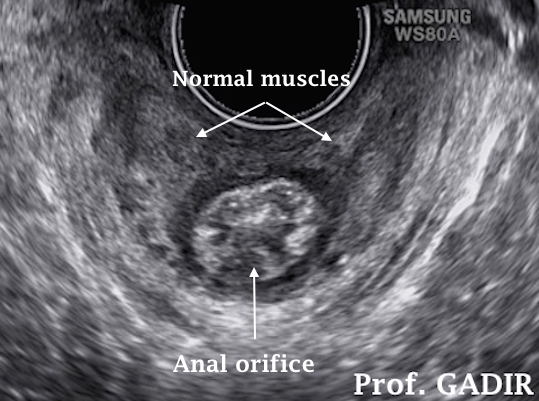
The third image is a similar view to the second one, which belongs to a multiparous women who did not have similar surgery. This image is shown for comparison reason.
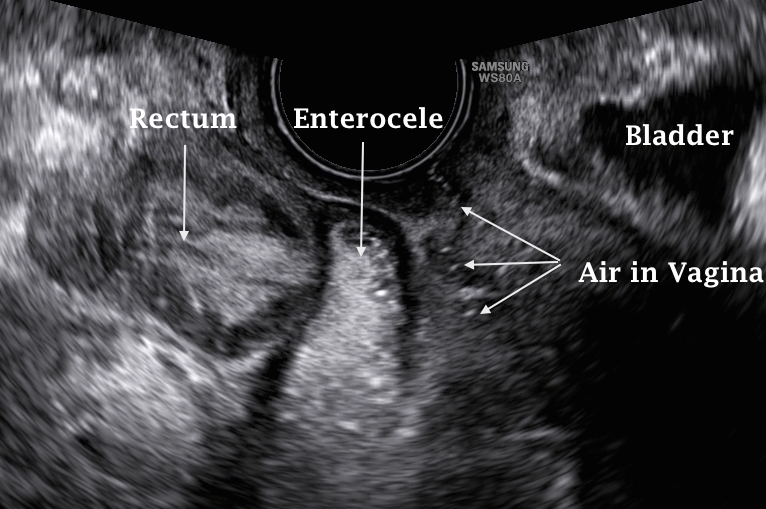
The role of ultrasound in the diagnosis of genital prolapse is beyond the scope of this basic review. However, the image below shows a great potential for transperineal scanning in this field. A large hernia of the pouch of Douglas is occupied by large enterocele reaching far down behind the vagina, in front of the rectum.
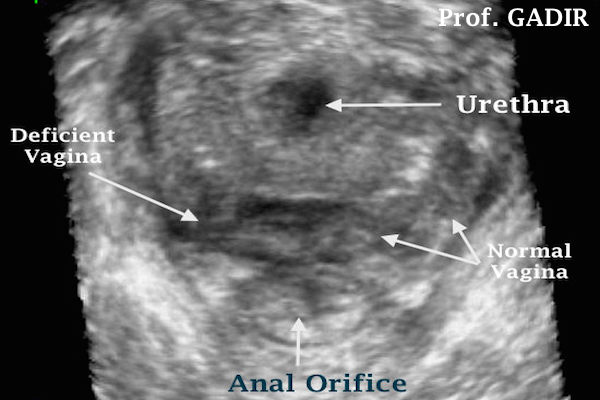
It is important not to forget the potential role of transperineal 3D ultrasound examination in the diagnosis of anal, lower vagina, and forchette muscular damage. The 3D magnified image shown below explicitly shows normal anal orifice, vagina and urethral meatus. Deviation form this normal shape will indicate some sort of damage. Such damage is shown in the second image below. It depicts perineal deficiency on the right side, with the vaginal wall dipping posteriorly rather than anteriorly.
Tranvaginal pelvic scanning
Technique
Pelvic scanning should be started in the anterior-posterior (AP) plane, before rotating the probe into thetransversepelvic plane.
In the mid AP position, the pelvis is examined in the sagittal view. Moving the probe to the right or left in the same plane will give right and left AP pelvic views respectively.
On the other hand scanning in the transverse pelvic plane is done when the probe is rotated 90o to the right or left to give the right or left transverse pelvic views respectively.
The uterus can be examined in AP (including sagittal) or apical (transverse pelvic) views, but never in a transverse uterine view during transvaginal scanning. It is only possible to have a transverse view of the uterus during transabdominal scan examinations when the scanning plane is perpendicular to the long axis of the body. This orientation is not possible vaginally.
Special note
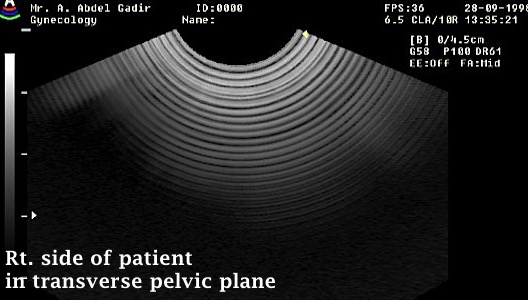
During transverse pelvic scanning, the right side of the monitor always corresponds to the right side of the patient, as shown in the image below. However there is no standardisation for AP scanning. This is left for the operators' choice and can be selected by setting the monitor.
The urinary bladder
The urinary bladder should be empty during transvaginal scanning. However when partly filled it shows a triangular shape in the sagittal view, but its outline may be dented by any uterine or ovarian mass pushing on its wall. The course of the urethra and the presence of bladder wall pathology, pararuretheral or vaginal cysts can easily be ascertained, with the probe inserted just into the lower vagina. This can be useful when investigating patients with urinary symptoms. The bladder wall thickness may be a useful finding in women with urinary symptoms especially with urgency incontinence. Other pathologies may also be seen.
The 3 images shown above depict:
Transverse pelvic view of bladder, urethra and 3 pararurethral cysts
Oblique view showing a suspected bladder wall endometriotic nodule
Thick posterior bladder wall in a patient with severe urinary urgency
The 3 images shown above depict:
Bladder showing turbid urine in anteroposterior and transverse pelvic planes. Turbidity can be seen on image magnification
Bladder wall split into two portions by a diverticulum.
3D findings in the same patient shown in the second picture, proving the presence of a large diverticulum
The cervix
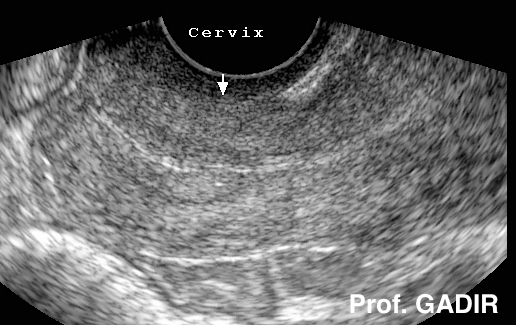
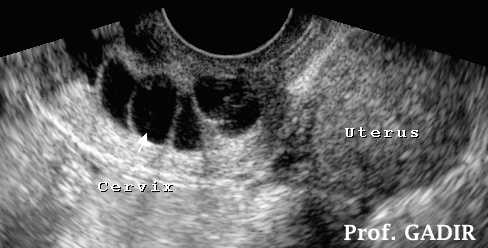
It is best to examine the cervix in the AP or longitudinal view during the periovulatory period. The cervix is 4 cm in average length, and is more echogenic than the rest of the uterus. Measurements less than 2.5 cm may have clinical significance during investigations of recurrent miscarriages. However, gradual shortening and funnelling during pregnancy are be more important than a single measurement.
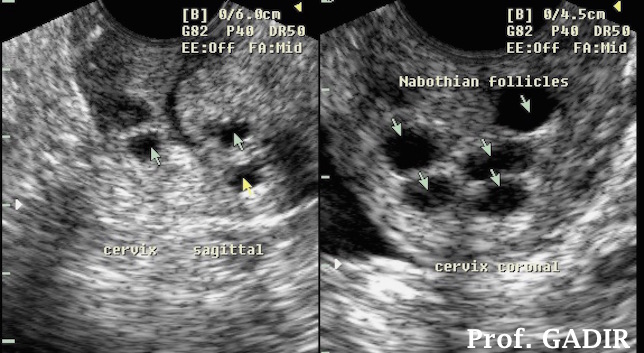
Nabothian follicles are frequently seen and can give a honeycomb appearance. During the reproductive years the cervix is normally shorter than the long axis of the body of the uterus and more echogenic. With the continuous decline in the uterine size during the postmenpausal years, the cervix and the body of the uterus may have the same length, or the cervix may even be longer.
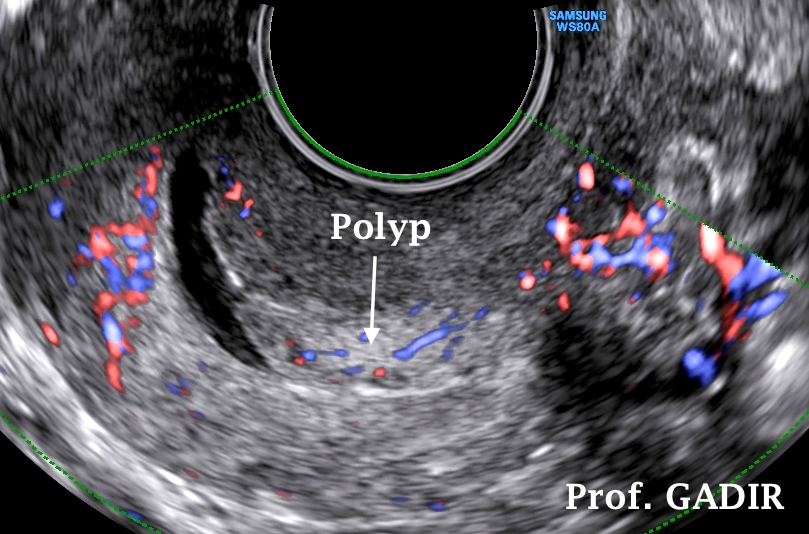
The presence of mucous in the endocervical canal during the periovulatory period helps with the diagnosis of intracervical polyps. Such polyps may present with intermenstrual or postcoital bleeding. Other pathologies which may affect the cervix include:
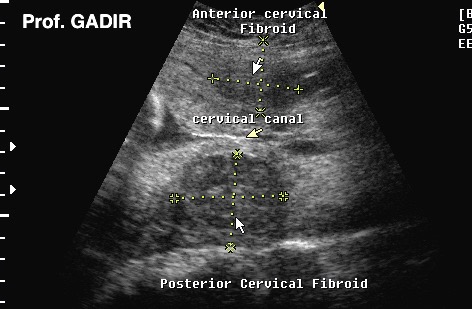
Cervical fibroids which may lead to difficulties during childbirth
Cervical ectopic pregnancies seen as dilated barrel shaped cervix.
Cervical carcinoma seen as a bulky and irregular cervix with undetectable cervical canal. Colour Doppler studies can show bizarre vascular arrangements within the suspected area.
The above 3 images show:
Longitudinal view of a normal looking tubular cervix
Longitudinal view of the cervix showing multiple nabothian cysts along the whole length of the cervical canal
Longitudinal and transverse views of a cervix showing multiple nabothian cysts in honeycomb appearance.
The above three images show:
Longitudinal view of a cervix showing an endometrial polyp with some mucous in the endocervical canal. Presence of mucous helps in polyps identification. A feeding vessel is seen passing into the polyp.
Longitudinal view of a cervix showing anterior and posterior cervical fibroids clamping the cervical canal. This patient was delivered by lower uterine segment caesarean section.
Oblique image of the uterus and cervix during saline infusion hysterography showing a large posterior cervical wall fibroid.
At this point, it is important to stress the fact that transvaginal scanning is not a recognised tool for cevical cancer screening or diagnosis. However, the presence of a cervical mass with bizarre blood flow, as depicted with power Doppler mapping, should raise the suspicion for such a diagnosis, as will be shown in Doppler section of this book.
The uterus
The uterus takes a central place in pelvic scanning. Although it is usually a midline structure within the lesser pelvis, deviations to one side or another are not uncommon. Its position (flexion and version), size and myometrial morphology should be noted. Unlike transabdominal scanning it is not usual to see the uterus and the cervix in the same plane during transvaginal scan examinations, except when using wide angle probes.
Version indicates the relationship of the long axis of the cervical canal to the long axis of the patient's body. Anteversion and retroversion are diagnosed when the lower cervix points backward toward the rectum, or foward toward the bladder respectively. In other words, with anteversion the external os points toward the floor and with retroversion the external os points toward the roof, in women in the lithotomy position.
Flexion reflects the relationship between the long axis of the body of the uterus to the long axis of the cervical canal. Anteflexion and retroflexion are terms used to indicate the fundus pointing forward toward the bladder, or backward toward the rectum ,respectively.
The indiscriminate interchangeable use of the terms version and flexion should not be allowed. The importance of such misnomenclature is demonstrated by cases of retroverted anteflexed or anteverted retroflexed uteri which are important causes of difficult embryo transfer and office hysteroscopy procedures.
The first ultrasound image below shows anteverted / retroflexed uterus. On the other hand the second image shows a retroverted / anteflexed uterus. The acute uterocervical angle in the second picture is demonstrated by the third 3D image showing the cervix and the top of the fundus both pointing forward with an acute angle in between [cochleate uterus]. This pattern we showed to be more common in nulliparous non-caucasian women in an article we published few years ago in 'Gynaecological Surgery'.
The myometrium
Normally the myometrium has homogeneous medium echogenicity which may be disrupted by such conditions as adenomyosis or fibroids. It is made of 3 layers, the middle one being the widest. The outer layer contains the subserosal blood vessels, and the inner hypoechoic layer has a clear interface with the endometrium. Disruption of this interface takes special importance when adenomyosis or malignancy are suspected in patients with relevant symptoms. Vascular markings can be seen toward the periphery, especially in parous women, and during pregnancy. They should not be mixed with other pathologies, like adenomyosis.
Uterine size
A normal uterus has different dimensions during adult life depending on parity and oestrogen status, as shown in the table below. Furthermore, uterine size increases by 3.2% and 1.8% every day during the follicular and the luteal phases respectively, but regains original size during menstruation.
Patients profile
uterine length
uterine width
uterine depth
Nulliparous
6 - 8 cm
3 - 5 cm
3 - 5 cm
Parous
8 - 10 cm
5 - 6 cm
5 - 6 cm
postmenopausal
3 - 5 cm
2 - 3 cm
2 - 3 cm
Beside these changes in size, uterine echogenicity also changes progressively after the menopause, reflecting changes in tissue texture, which may have similar echogenicity to the neighbouring structures.
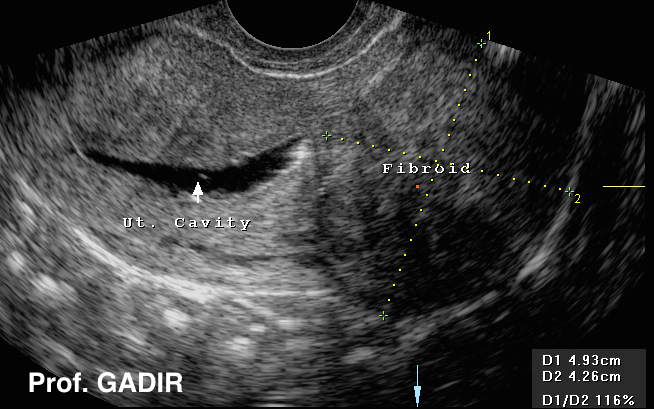
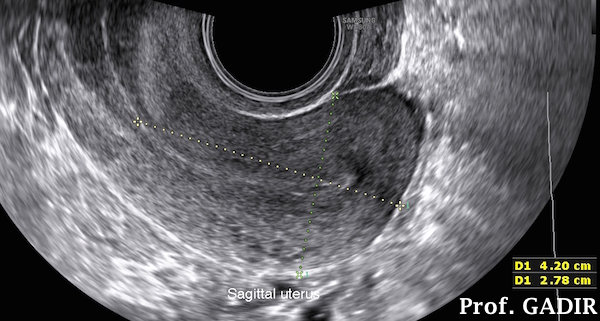
The above image first shows measurement of the body of the uterus, excluding the cervix, starting at the level of the lowest part of the uterovesical fold, up to the fundus. The hight is taken at the widest part of the body of the uterus, across the longitudinal plane.
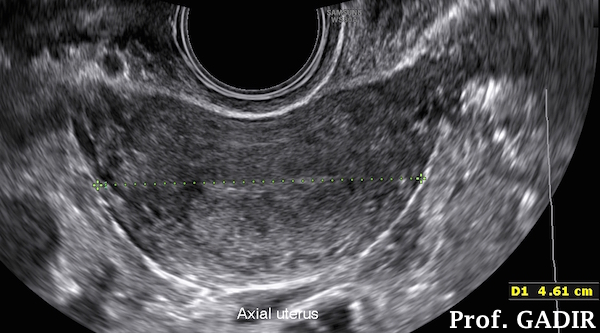
The second image shows measurement of the width of the uterus at the widest part across the fundus.
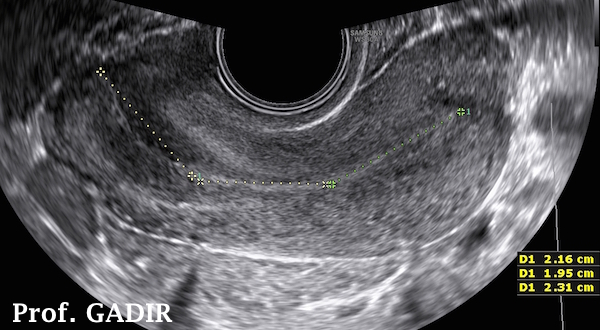
The third image shows measurement of the exact uterine cavity and cervical canal length, put together.
The uterine volume can be calculated from the equation:
Length x hight x width x 0.523
Uterine anomalies
With new machines with 3D capabilities, uterine shape can be ascertained easily. This was not possible previously, and either hysterosalpingography or diagnostic laparoscopy wa needed to ascertain such congenital uterine abnormalities. Such problems may result from:
Failure of fusion of mullerian ducts
Arcuate uterus
Bicornuate uterus
Double uterus
Failure of canalisation of the genital tract after fusion of the mullerian ducts
Complete septatum
Incomplete septum
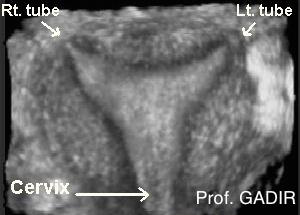
The 3D images shown above depict the following findings respectively.
An arcuate uterus with minimal dent of the top of the cavity and an intact fundus
A uterus with complete septum and intact fundus
A uterus with incomplete septum and intact fundus
A unicornuate uterus showing a banana cavity after saline infusion sonohysterography
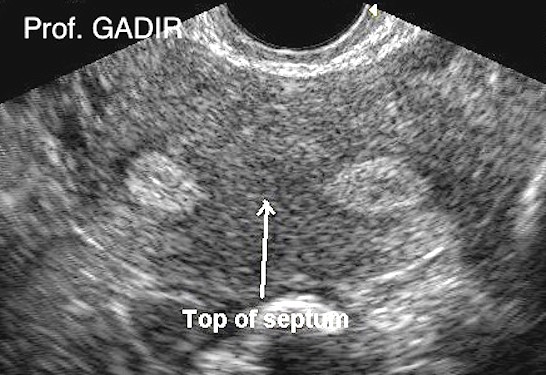
It is not always necessary to use 3D to diagnose a subseptate uterus. Having an axial view of the uterus in the transverse pelvic plane can show two circular endometrial areas, separated by muscular tissue, which is the septum. The fundal area will also be intact or minimally dented. This picture may be more evident during the luteal phase of the cycle, as the echogenic endometrium will stand out, against the less echogenic myometrium.
The two ultrasound images above show axial views of the same septate uterus near the fundus [left], and towards the lower end of the septum [right], where the two horns almost meet each other, as marked with an arrow.
Caesarean section scar
Special attention showed be paid to caesarean section scars during uterine examination. Occasionally a wide niche may be seen which necessitate 3D ultrasound examination to verify its extent. Please see the side menu for the chapters titled Fibroids and adenomyosis to complete the picture for uterine pathology.
The first image above shows an intact caesarean section scar marked by arrows. The second image shows a wide caesarean section niche. The third image is a 3D view of the same uterus shown in the second picture. It shows almost complete dehiscence of the caesarean section scar. The cervix is also shown as a dark area. This patient presented with persistent intermenstrual bleeding mostly due to retention of the menstrual blood within the scar hiatus and its intermittent release after cessation of menstruation. Resuturing the dehiscent scar corrected the intermenstrual bleeding.
The endometrium
Th endometrium is a dynamic tissue which constantly changes texture during the cycle. Normally a very thin endometrial line will be seen on each side of the cavity by the end of menstruation. A thick endometrial echo at this stage is usually suggestive of endometrial pathology, polyps or submucous fibroids. A normal endometrium can measure up to 12 mm during reproductive years.
When assessed at midcycle, the endometrium is usually hypoechoic and trilaminar in shape. This facilitates the diagnosis of echogenic polyps splitting the central echo. Submucous fibroids, on the other hand, are more hypoechoic and tend be seen better pushing the echogenic secretory endometrium. On the other hand intrauterine adhesions can be seen as:
Irregular or indiscriminate endometrial line
Thin endometrium despite good ovulation
Bright echogenic bridges across the endometrium
Previous history of uterine surgery, or infection following a pregnancy can usually be elicited in these case. Saline infusion sonohysterography may be the best method for confirming the diagnosis. More information can be found in the chapter titled hypomenorrhoea, on the side menu.
The first image above shows sagittal and axial views of a uterus with thin menstrual endometrium, and some blood in the cavity.
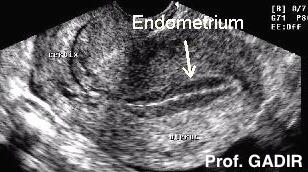
The second one shows midcycle trilaminar endometrium, with 2 hypoechoic areas between the 3 sharp lines. The central echo denotes the cavity and the line of contact between the two endometrial surfaces. Such a straight unbroken line excludes the presence of polyps.
It remains to be said that the endometrium may be thick, heterogeneous with irregular outline and fluid or debris in the cavity in cases of endometritis. This picture should be correlated to the clinical presentation. Similar findings may be seen in cases of endometrial malignancy in postmenopausal women with abnormal uterine bleeding. Obesity, nulliparity, late menopause and use of unopposed oestrogens increases the risk of such a malignancy. On the other hand the endometrium may be diffuse and thick with intact interface with the myometrium in cases of hyperplasia, and at the base of broad based polyps. An irregular endometrial / myometrial interface can also be due to focal adenomyosis, with the ectopic endometrium pushing through the junctional zone.
Endometrial thickness should be assessed in the longitudinal [sagittal] uterine plane, and the thickest area of the endometrium should be measured. It is important not to include the hypoechoic junctional zone of the myometrium into the measurement.
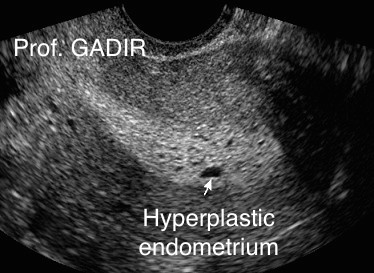
The first image above shows hyperplastic endometrium with intact interface with the neighbouring myometrium. The diagnosis was confirmed histologically. The second image shows thin endometrium with echogenic area under the caesarean section scar. This patient presented with secondary amenorrhoea due to intrauterine adhesions following the caesarean section.
It is important to note that 2D diagnosis of hyperplastic endometrium may not be right all the time. A provisional diagnosis of hyperplastic endometrium was made when one of our patients was first scanned, as shown by the first combined 2D image above. Using 3D, as seen in the second image above, showed multiple fundal endometrial polyps. The diagnosis was also confirmed histologically in this case. This case emphasises the need to use 3D technology in all cases with abnormal uterine findings on 2D scanning.
Clinical value of endometrial thickness
An endometrial thickness < 5 mm almost excludes the risk of malignancy in cases of postmenopausal bleeding. However a figure up to 8 mm could be normal in obese women, patients on HRT and hypertensive women taking calcium channel blockers. A thick endometrium in non-symptomatic postmenopausal women should not indicate invasive treatment as bleeding is usually the first symptom of malignancy. Such thick endometrium could be due to an endometrial polyp as an example. At the same time endometrial thickness does not carry the same diagnostic weight of sinister pathology in younger symptomatic women within their reproductive age as for postmenopausal ones.
In summary endometrial pathology could be reflected by one of the following findings:
> 5 mm thick endometrium at the end of menstruation,
abnormaly thick endometrium > 13 mm at other times of the cycle,
abnormally thin endometrium at midcycle,
irregular endometrial / myometrial interface,
indiscriminate endometrial outline,
heterogenous endometrial texture.
The presence of fluid in the uterine cavity could be seen in the following conditions:
during menstruation,
during super-ovulation,
incomplete miscarriage,
cervical stenosis,
endometritis with irregular heterogenous endometrium,
cervical or endometrial cancer.
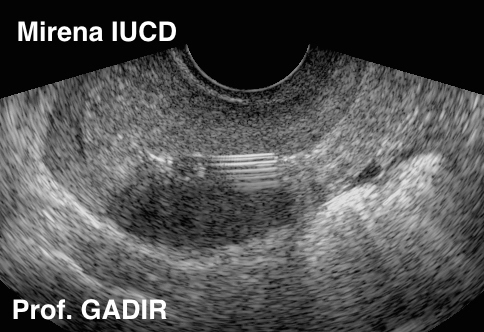
It is not an usual to receive requests for scanning patients for localisation of intrauterine contraceptive devices. Different devices have different looks and some times 3D ultrasound or plain X ray may be necessary for that purpose.
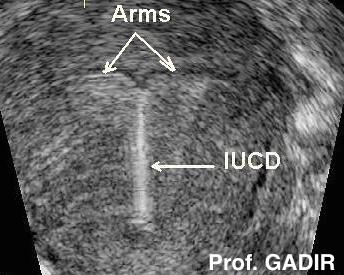
The first image above shows a bright copper IUCD with a strong shadow underneath. The second image shows a characteristic look of the less echogenic mirena IUCD and the third image is a 3D view of a uterus with an IUCD arms penetrating through a caesarean section scar. The body of the IUCD was still in the cervical canal. This last picture belongs to a patient who presented with persistent bloody vaginal discharge. She had no pain despite the device penetrating through the caesarean section scar.
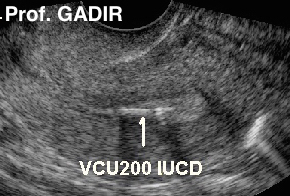
The value of 3D imaging is further shown by the three ultrasound images shown above. A 48 year old woman presented with intermittent abnormal uterine bleeding and brown discharge for few months. Transvaginal ultrasound scanning was depicted by the first image above. It did not fit into any of the IUCD types the author has used or seen before. The second one is a 3D image which showed an IUCD that proved to be a long forgotten by the patient VCu200 intrauterine contraceptive device, which she has been wearing for many years. Compare this 3D image to the neighbouring 3D image which showed a normally positioned copper IUCD with both arms stretched as expected across the fundal area of the uterus.
The ovaries
The ovaries can be seen between the uterus medially and the internal iliac vessels laterally, which are good landmarks posterior and lateral to the normally sited ovaries. Occasionally, they may be displaced temporarily in front or behind the uterus. In case of difficulty, scanning along the internal iliac artery may be helpful, as they are often located anterior to its bifurcation, into its anterior and posterior branches. Permanent dislocation of the ovaries out of their usual sites, is indicative of pelvic adhesions. Occasionally, one or the other ovary may be closely attached to the uterus. This may, as well, be a sign of pelvic adhesions. Pushing with the vaginal probe, usually allows the ovary and uterus to move in different directions. In case of adhesions, they both move along the same direction. This test is known as organs sliding test, and is usually negative in case of adhesions.
As for the uterus, ovarian size depends on age and endocrine status. The expected average ovarian volume during the reproductive years would be 5.0 - 9.0 ml and they have symmetrical size and characteristic appearance depicted by the presence of few antral follicles within an ovoid structure. Ovarian size before menarche and after the menopause would be around 3 ml. Calculation of ovarian volume is mostly given directly by modern ultrasound machines after recording length, breadth and depth. However, multiplying the 3 measurement by a factor of 0.523 could also be used to calculate ovarian volume. A small ovary < 2 ml with no follicular activity wihin the reproductive years is usually diagnostic of premature ovarian failure. On the other hand a polycystic ovary might be >10 ml in volume. In such cases > 12 small cysts < 9 mm in diameter would be seen either subcapsularly or dispersed over the stroma. Such pattern is seen in women with polycystic ovarian syndrome but is not diagnostic of the condition in isolation. Polycystic ovaries could be seen in women with thyroid problems, hyperprolactinaemia, 21 hydroxylase deficiency as well as in 20% of normal women with no endocrine, menstrual or fertility problems.
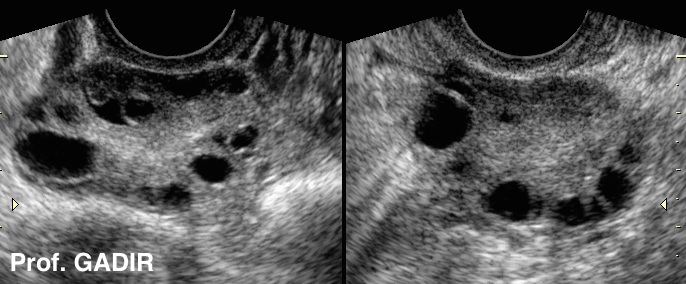
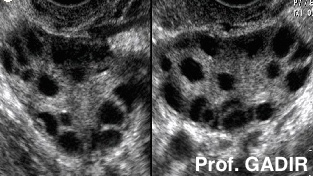
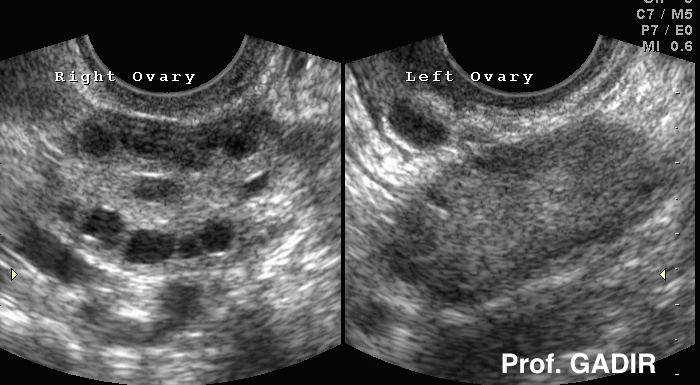
The first 2 images shown below depict subcapsular and stromal distribution of the small cysts respectively. The third image shows unilateral polycystic ovary with a normal contralateral one. All 3 patients were hyperandrogenic with anovulatory problems.
After the menopause there is a gradual decline in ovarian size and follicular activity with time. It is important to remember that up to 25% of women within the early postmenopausal year might show simple follicular cysts < 5 cm in diameter. These patients should be followed with repeated ultrasound scan examinations so long as there is no indication for immediate or subsequent surgical intervention [see ovarian cyst on the side menu]
Displacement of one or both ovaries and significant discrepancy in their size could indicate a pathological condition worth of further investigations. One or both ovaries could be displaced due to uterine retroversion or by pelvic adhesions. Transvaginal ultrasound scanning might fail in revealing these ovaries if they were displaced high behind the fundus of the uterus. In such cases abdominal pressure with the free hand could bring the ovary within reach or transabdominal scanning might be needed to examine that displaced ovary. Other signs of adhesions include encysted fluid in the pelvis, dilated fallopian tubes and failure of the ovaries and uterus to move in different directions during pressure with the probe [negative organs sliding test]
Different types of cysts could change the overall size and texture of the ovaries. Ovarian pathology is best seen during the early follicular phase.After the menopause the ovaries tend to get smaller, hypoechoic and difficult to locate. Occasionally only the right ovary is accessible as the left one might be masked by bowel shadows on the left side. They could also show bright echogenic shadows which are mostly haemosidrin deposits and calcifications. More information would be found in the 'Ovarian Cysts Chapter in this website.
The fallopian tubes
Further assessment of the pelvis should include the fallopian tubes, which are not usually visible in normal circumstances. However, the fimbrial end may be seen when there is some fluid in the pelvis, especially if the patient is put on a semi-sitting position. Furthermore, normal tubes can be seen if an echogenic fluid is instilled into the uterus [see HyCoSy on the side menu]. Nevertheless, it is not usually possible to see the whole length of the tube in one plane. A normal tube is 8-12 cm long and has 0.5 mm internal diameter at the interstitial part but up to 1.5 mm in the fimbrial part. Thickening of the wall or dilatation of the lumen with fluid, ectopic pregnancy or a mass would make them more readily visible. A dilated tube is usually retort shape structure beside the uterus with one or more incomplete septae [pseudo septae]. Such hydrosalpinges are best seen during the mid cycel before they drain back after ovulation, becuase of the progesterone induced relaxation of the tubo uterine junction [communicating hydrosalpinges]. On the othe hand tubal ectopic pregnancies are best seen in the 'ectopic angle' between the uterus and the epsilateral ovary harbouring the corpus luteum [see ectoptic pregnancy on the side menu].
Ultrasound may also be very useful in differentiating between acute and chronic salpingitis. In the acute type, the tubes are usually thick and oedematous, and may contain some fluid. A cross section view may give a Cogwheel Appearance due to swelling of the tubal folds. In contrast, in chronic salpingitis the tube wall is thin. Chronic tubal dilatation usually leads to atrophy of the inner folds resulting in Pearls on the String appearance. The difference between the two conditions is depicted by the two ultrasound images shown below.
Furthermore, ultrasound scanning is important to differentiate between tube-ovarian complex and tube-ovarian abscess. In the former one the ovary and tube can be differentiated separately, whereas in the later pathology no line of demarcation can be seen between the two. This is important, as antibiotics are necessary for the tube-ovarian complex, where as an abscess needs draining plus the antibiotic cover.
The Pouch of Douglas
Examination of the pouch of Douglas may show free or encysted fluid during reproductive years. Such fluid is normally clear but may be turbid, if it contained blood or pus cells. Patients with endometriosis may also show more fluid in the pouch of Douglas compared to normal women. Occasionally, a woman may present with acute pelvic pain related to a ruptured ovarian cyst. In such cases a collapsed ovarian cyst may be seen with excessive amount of free fluid in the pelvis. Tenderness may be an important feature during transvaginal scan examination, while moving the probe.
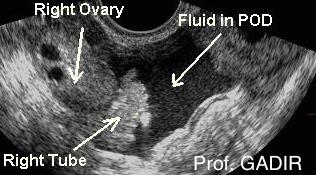
The first image above is a transverse pelvic view showing fluid in POD with the right ovary and fimbrial end of the right tube clearly seen
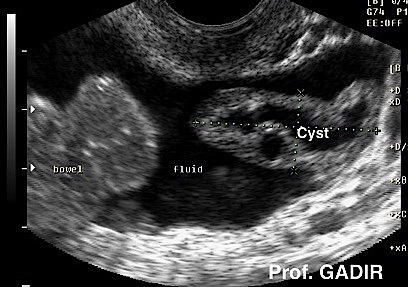
The second image shows a collapsed left ovarian cyst wall with a lot of fluid in the pouch of Douglas and floating bowel nearby. This patient presented with acute pelvic pain cause by spontaneous rupture of a left ovarian cyst.
Moderate or excessive of fluid in the pelvis following the menopause should raise the suspicion of pathology, mainly ovarian cancer and hepatic disease. Rectovaginal endometriosis and pelvic abscesses, may as well, be seen as heterogeneous masses in the POD. Clinical presentation usually helps in making the diagnosis.
The 2 transvaginal ultrasound images shown above depict respectively:
Sagittal view of the uterus showing obliteration of the pouch of Douglas with rectovaginal endometriosis.
An oblique view showing a lateral wall vaginal cyst, the urethra and part of the urinary bladder.
For further information regarding the use of ultrasound in diagnosing gynaecological pathology please refer to the chapters entitled Fibroids, Ovarian Cysts, Adenomyosis, Endometrial Polyps, Ectopic Pregnancy, Pelvic Congestion Syndrome, Saline Infusion Sonohysterography, and HyCoSy.