This is a term used to indicate significant reduction in menstrual blood flow compared to the patients usual pattern or menstruation lasting for less than 2 days. It could follow prolonged use of any monophasic contraceptive pill or a mirena device because of their dominant progestational effect on the endometrium. Progestogens usually downregulate their own as well as oestrogen receptors and lead to progressive atrophy of the endometrium. A higher dose of oestrogen would be needed to stimulate endometrial growth with such dominant progestational effect. This is very clearly demonstrated in patients who receive oestrogen medication to treat abnormal uterine bleeding caused by prolonged use of depo provera injections. However, hypomenorrhoea might have special anatomical significance if it followed any pelvic surgery or infection involving the uterine cavity. In these cases intrauterine adhesions should be suspected. Many patients might present with scanty menstrual flow. Others may present with amenorrhoea altogether. Trauma to the endometrium could follow such conditions as:
D&C
Evacuation of the uterus
Lower uterine segment caesarean section
Manual removal of the placenta
Myomectomy
Genital tuberculosis in certain parts of the world can cause hypomenorrhoea or amenorrhoea not responsive to hormonal treatment. This can lead to formation of intrauterine adhesions [Sharma et al, 2008], or total damage of the basal endometrial layer by the tuberculosis granulomas. These may not be easily retrievable with the curette, as they tend to be near the vicinity of the inner fallopian tubes ostia.
It is noticeable that pregnancy is a common factor in most of these cases with superimposed infection being the direct cause leading to adhesions formation. Furthermore, more adhesions follow evacuation of missed than incomplete miscarriages. The uterine pathology could be:
Complete or partial obstruction of the uterine cavity with adhesions.
Apical adhesions covering the area of the internal cervical os only.
Damage to the basal endometrial layer without any adhesions formation.
In managing these cases previous history could be the most important diagnostic clue especially if the symptoms followed an operative procedure. On the whole, systemic and pelvic examinations would be unremarkable. However transvaginal scanning could show:
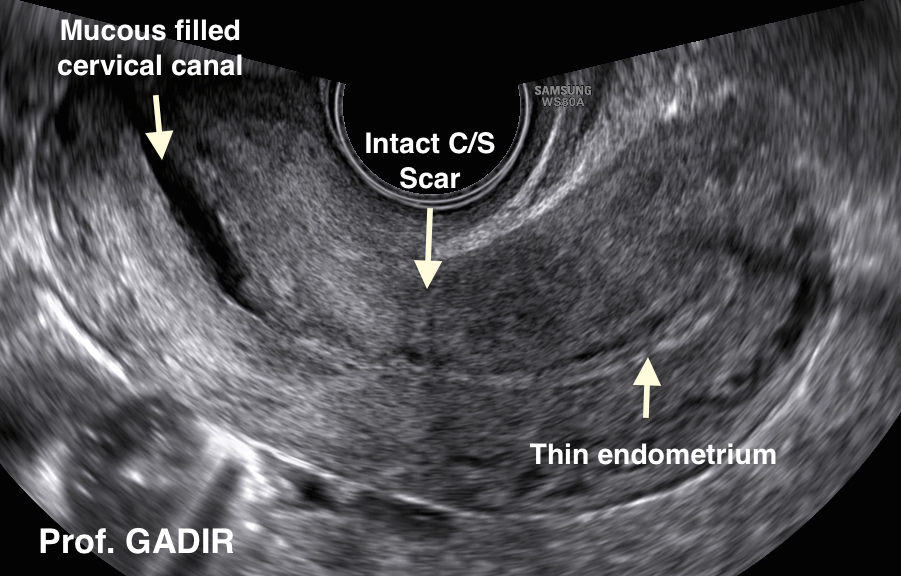
Thin endometrium even when stimulated with exogenous oestrogens.
Bright intrauterine echoes due to scar tissue bridges.
Indiscriminate interface between the endometrium and myometrium.
The first image above shows mucous filling the cervical canal, yet with very thin endometrium following external stimulation with oestradiol benzoate for two weeks. This patient had hypomenorrhoea after lower uterine segment caesarean section. The endometrium otherwise was unremarkable, and the caesarean section scar was intact. In this case partial damage of the basal endometrial layer was suspected, as hysteroscopy showed no adhesions.
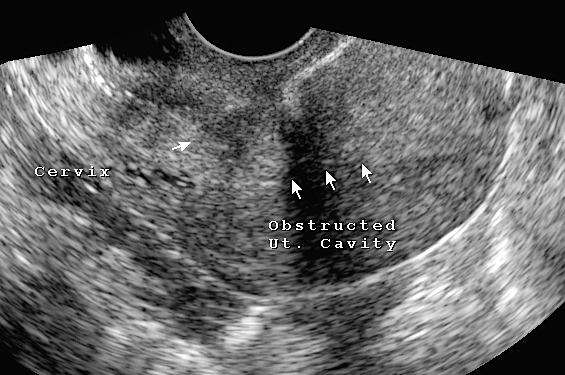
The second image showed total endocervical and endometrial obliteration. A stiff catheter failed to negotiate the endocervical canal, hence saline infusion could not be done.
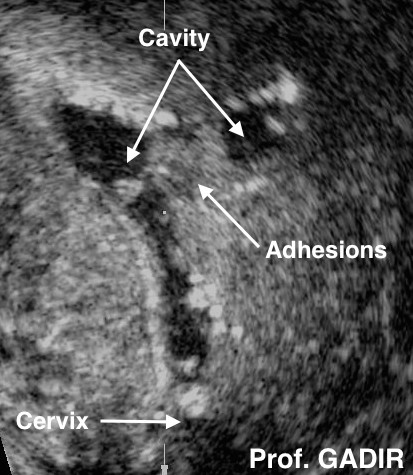
The third image showed mid uterine cavity adhesions. Very little saline managed to reach the upper cavity after sonohysterography. This patient also presented with hypomenorrhoea and intermenstrual bleeding, mostly due to lower cavity obstruction.
Using saline infusion sonohysterographymay confirm the diagnosis and show the extent of intrauterine adhesions as shown below. Hysteroscopy is another method for diagnosing and treating these adhesions.
The first 2D picture above shows an irregular uterine cavity after saline infusion sonohysterography. The second picture is as 3D rendered view showing intrauterine adhesionS occupying most of the left side of the cavity. The patient presented with very light menstrual periods after an open myomectomy. This rendered view was very helpful in directing the hysteroscopic procedure, and showing how much tissue had to be removed. This patient resumed menstruating and managed to conceive naturally.
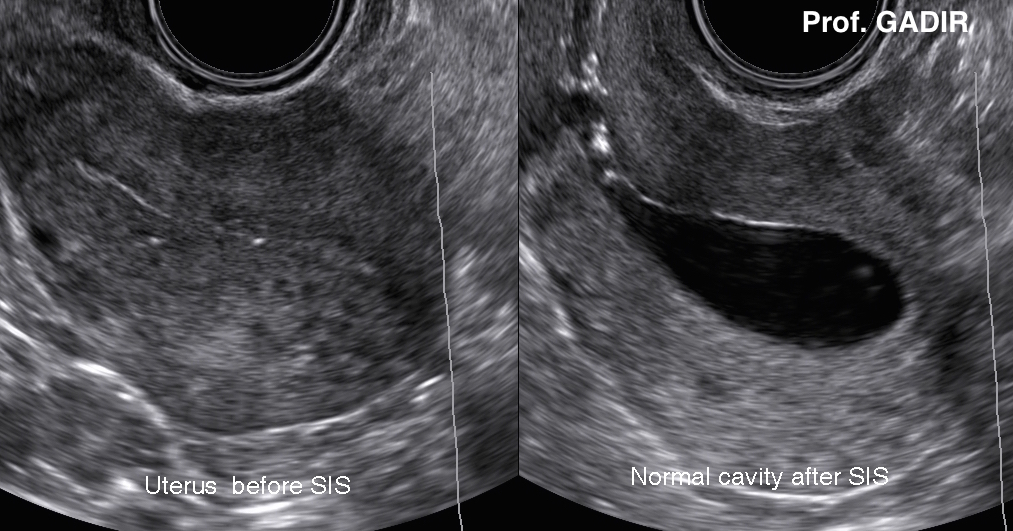
However, occasionally saline infusion hysterography may show a normal looking uterine cavity despite an initial diagnosis of indiscriminate endometrial / myometrial interface as shown by the two images below. This patient gave no previous history of any intrauterine surgical procedures, or pelvic infection. There was family history of tuberculosis, though she tested negative herself. She did not have a good endometrial response to exogenous oestrogens medication. Her thin endometrium and severe hypomenorrhoea remained unexplained. She left the clinic before further investigations could be done.