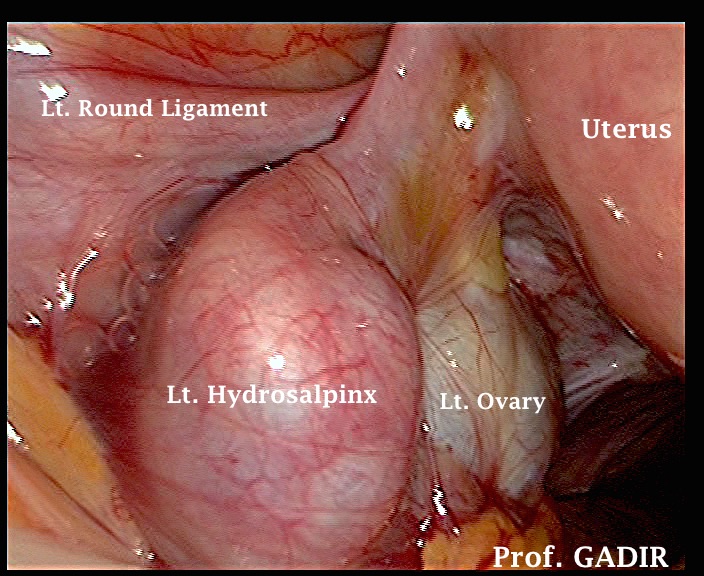
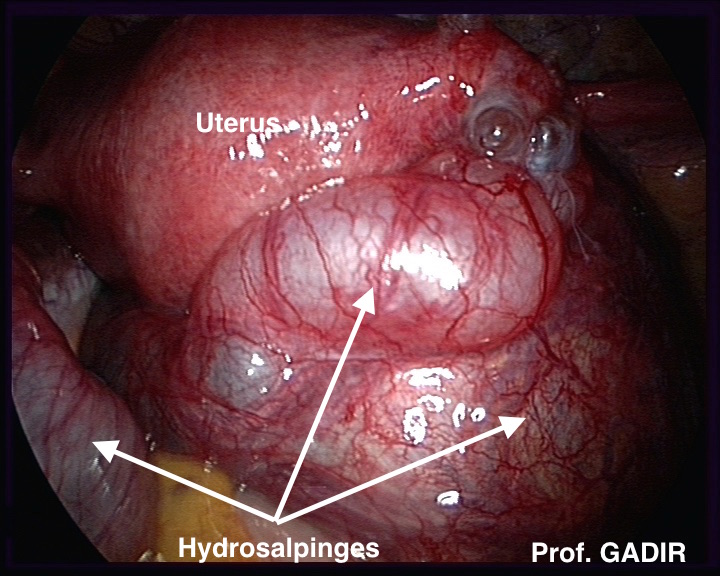
The laparoscopic images shown above depict how dilated tubes look in real life. These images may help ultrasonographers who are not normally involved with laparoscopic surgery to have a real visual image when they are performing ultrasound scan examinations. It is important to remember that HSG may give false results with tubal patency. A large hydrosalpinx may allow spread of the dye into the dilated distal part of the tube, simulating proper smearing as seen with normal tubes. I have seen this problem on few occasions when HSG reports document patent tubes where as transvaginal scanning confirmed the presence of large hydrosalpinges. Unfortunately most clinicians not personally involved in scanning their own patients tend to follow the result of the HSG.
It is very easy to diagnose a hydrosalpinx with transvaginal scanning using 3 diagnostic criteria :
-
Loculated clear fluid in the pelvis
-
The presence of incomplete septa within the dilated tube. This can be identified easily by scanning the tube in different planes by gentle rotation of the probe.
-
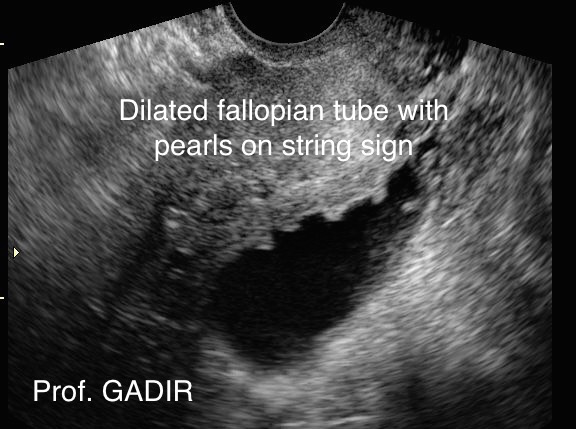
It has a retort shape with a waist sign as seen in the ultrasound picture below. However, the tube can be seen in multiple cross sections depending on the plane of scanning
- The first image above shows a dilated fallopian tube with a 'waist sign' seen as a constriction in the wall of the tube.
- The second image shows encysted fluid beside the fallopian tube indicating the presence of pelvic adhesions.
- The third image depicts a dilated tube showing 'Pearls on the String' sign which may be seen with chronic pelvic inflammatory disease
Dilated tubes may drain back into the uterus during the luteal phase rendering them less identifiable by ultrasound. This is secondary to relaxation of the interstitial part of the tube induced by progesterone. Such tubes are called Communicating Hydrosalpinges. Accordingly, pelvic scanning for tubal pathology may be more informative if timed to the pre-ovulatory phase of the cycle.
Hydrosalpinges and IVF
It is now an accepted fact that hydrosalpinges can significantly reduce pregnancy rate after IVF, hence they should be removed before starting such treatment.
However, the practice of clip application to block the promixal part of these dilated tubes should be discouraged. Continuous secretion of fluid secondary to the elevated oestrogen levels during IVF treatment may lead to gross enlargement of these tubes without a relief route for drainage. This could lead to the following 3 problems:
-
Difficulty during monitoring follicular growth in some cases due to ovarian displacement and the increased amount of fluid in the pelvis around the ovaries.
-
Increased risk of tubal torsion due to the gross lateral enlargement of the tubes with narrow proximal part.
-
Increased risk of infection after transvaginal oocytes collection leading to pyosalpinges formation with turbid / particulate fluid
Pelvic adhesions
Adhesions are bands of scar tissue which connect two or more organs together. They can form in the pelvis following surgical procedures or episodes of infection. They can be thin, membranous, thick, vascular or avascular and are usually graded into 4 stages of severity accordingly to their nature and extent of involvement of different organs. Different findings during ultrasound scan examinations may suggest the presence of pelvic adhesions. These signs include:
- Fixed retroversion of the uterus
- Dislocated ovaries
- Encysted fluid in the pelvis
- Dilated tubes
- Negative organ sliding test with restricted pelvic organs movement in relation to each other during examination
- Undue pelvic pain may be a sign of pelvic pathology, mainly pelvic inflammatory disease or endometriosis.
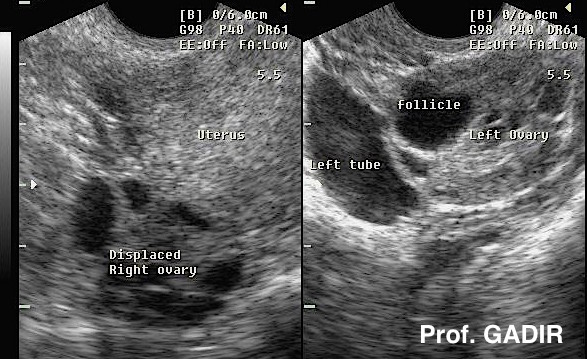
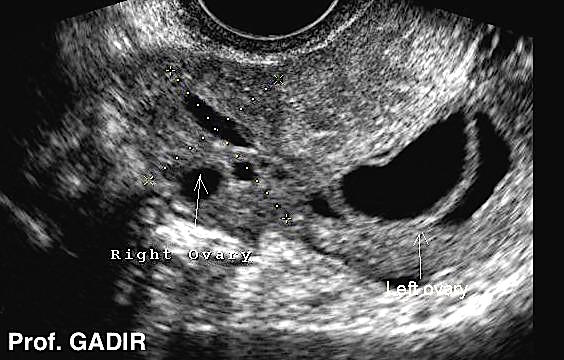
The first split 2D image above shows the right ovary displaced behind the uterus. The left ovary was normally sited, but was flanked by a dilated left tube. The second 3D image shows an ovary with loculated fluid in the pelvis, partly cross-setion of the fallopian tube, and partly encysted peritoneal fluid. The third image shows both ovaries lying behind the uterus in the cul de sac. These ovaries are usually stuck together with adhesions and are called 'kissing ovaries'.
Monitoring natural cycles
Serial ultrasound scan examinations during one or more menstrual cycles may add very important information, which can help in infertility management. Different issues are examined including:
-
Early follicular phase scanning can show how many antral follicles are present, which is an important point in studying ovarian reserve. On the other hand, multiple and rapid recruitment may be signs of incipient ovarian failure, especially in women with short follicular phase.
- Doppler examination of the subendometrial blood flow and uterine artery pulse wave studies give useful information regarding the blood flow within the uterus. As well peripheral vascularisation of a dominant follicle indicates imminent ovulation. A relationship has been recorded between unexplained infertility and high uterine artery pulsatility index. This has also been shown for anovulatory women with PCOS. Uterine artery pulse wave signature is recognised by the location of the arteries lateral to the cervix, the sound of the pulse produced by the artery, and last by the shape of the pulse wave itself.
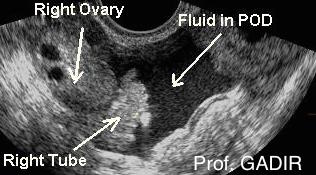
The first image above shows a uterus with midcycle trilaminar endometrium. The second image shows fluid in the pouch of Douglas which is a common finding at the time of ovulation. The third image shows an echogenic luteal phase endometrium.
Doppler and Pulse characteristics
Uterine arteries normally have high systolic blood flow, with a diastolic notch and high resistance. They are easily identifiable on each side of the upper cervix. On the other hand, ovarian vessels have low velocity with low diastolic flow during the follicular phase. Furthermore, they are difficult to locate and to have a good Doppler signal from, because of the suboptimal angle of insonation Accordingly, they are not historically utilised for diagnostic purposes. At the same time, resistance to flow is 40% lower in the intra ovarian vessels, compared to the main artery. More and above, pulsatility index is lower in the side carrying the dominant follicle or corpus luteum compared to the contralateral side.
The following changes in blood flow may take place at or after ovulation time:
- Maximum neovascularisation of the dominant follicle at the time of LH surge
- Increased velocity in uterine arteries and increased diastolic blood flow.
- Increased ovarian vessels velocity and decreased resistance
- Both vessels pulsatility indices are reduced after ovulation.
Though not universally proven, a uterine artery pulsatility index equal or less than 3 indicate good uterine perfusion.
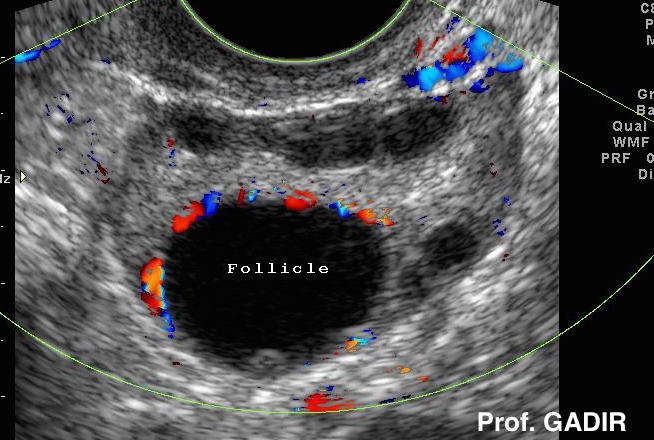
- The first colour Doppler above shows early vascularisation of a mature follicle, before LH surge.
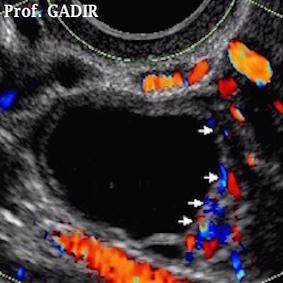
- The second colour Doppler image shows a polycystic ovary with a mature follicle showing good vascular rim.
- The third colour Doppler image shows double ovulation with a mature follicle with a rich ring of colour in the right ovary and a corpus luteum in the left side. This is an indication of a wide window of ovulation of two follicles ovulating at different times. This is more common in women over the age of 37 years, as one follicle does not produce adequate amount of oestradiol to stimulate the negative feedback mechanism, hence allowing more than one follicle to grow. This explains the higher rate of twins in this age group compared to younger women.