HyCoSy has already replaced X-ray hysterosalpingography [HSG] for fallopian tubes studies in many centres, avoiding the need for pelvic organs radiation. It is an office procedure associated with minimal discomfort. Nevertheless patients are advised to take two nurofen tablets one hour before the procedure. It is done during the follicular phase of the cycle between days 5 and 10 depending on the duration of the patients menstruation. Antibiotics prophylaxis is also necessary to cover the procedue
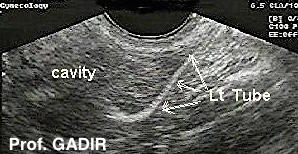
Following aseptic insertion of a ballooned catheter into the uterine cavity, the interstitial parts of both fallopian tubes are identified in the transverse pelvic plane.The contrast medium (Echovist) which is a sugar [galactose] solution is then injected slowly and each tube is identified by scanning out of the fundus and forward (anteriorly).The flow of the media for 10 seconds confirms tubal patency.
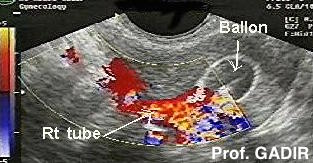
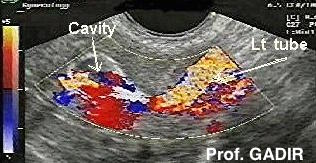
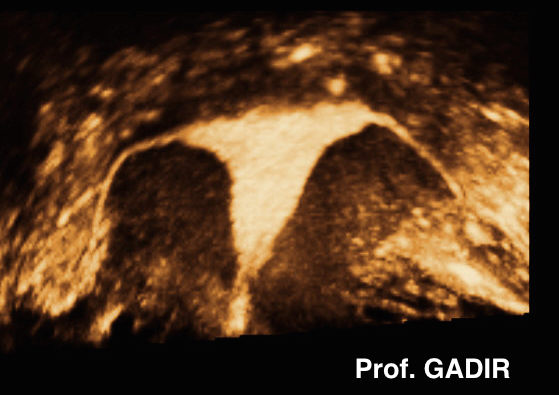
The top 2 images show the balloon in the uterine cavity and the left tube radiating up and out of the fundus. On the other hand, the lower 2 images show the right and left tubes after switching on the colour Doppler.
HyCoSy with colour Doppler is as accurate as hysterosalpingography in assessing tubal patencywithout subjecting a patient to any x-ray radiation. Though not needed in most cases, the importance of colour Doppler is well demonstrated in difficult cases with increased bowel shadows. We have been using colour Doppler as the routine practice in all cases when possible, to reduce the procedure time and the amount of fluid needed.
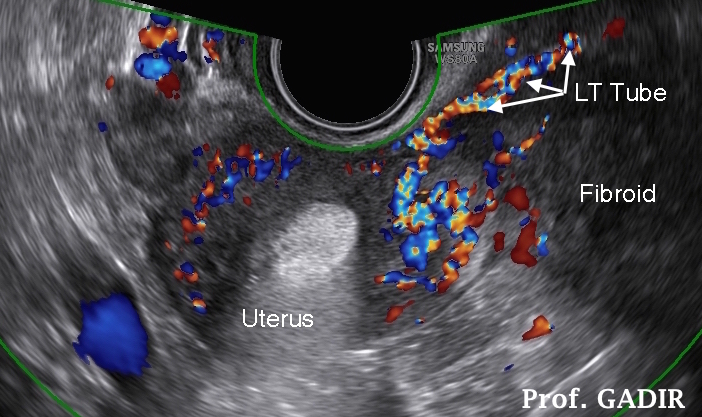
Another advantage of HyCoSy over HSG is the ability to examine the course of the tube relative to the corresponding ovary. Any tubal displacement following pelvic adhesions or the presence of broad ligament fibroid may be identified.
Furthermore, it can be combined with baseline ultrasound scan examination to detect any pelvic abnormality in those who have not been scanned before.
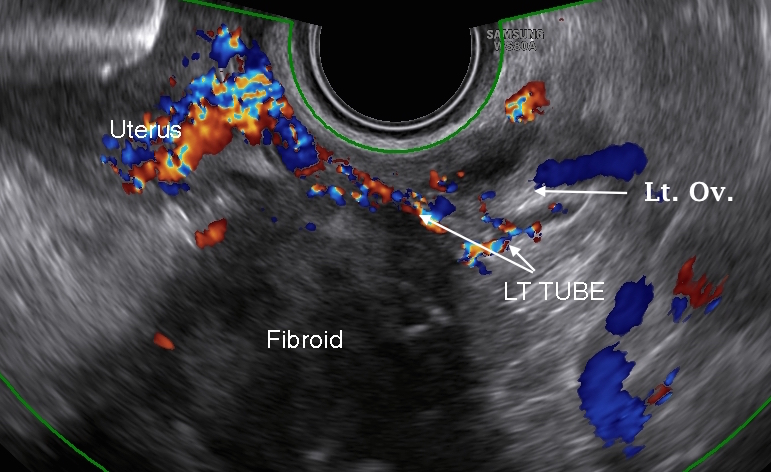
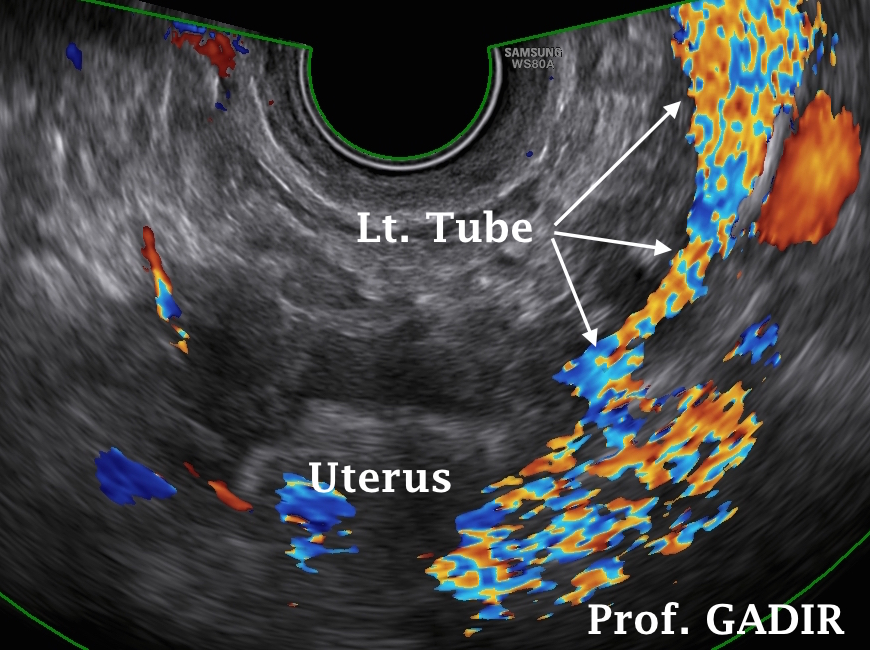
The first colour Doppler image above shows the proximal part of the left fallopian tube displaced by a left broad ligament fibroid. The second image shows continuous colour marking the tube running between the fibroid and the left ovary. Numerous snapshots at different levels were needed to document complete patency of the tube. This was helped by moving the probe to follow the flow of the foam. Only two of these images are shown in this text. Previous hysterosalpingography in this patient showed proximal block of the left tube.
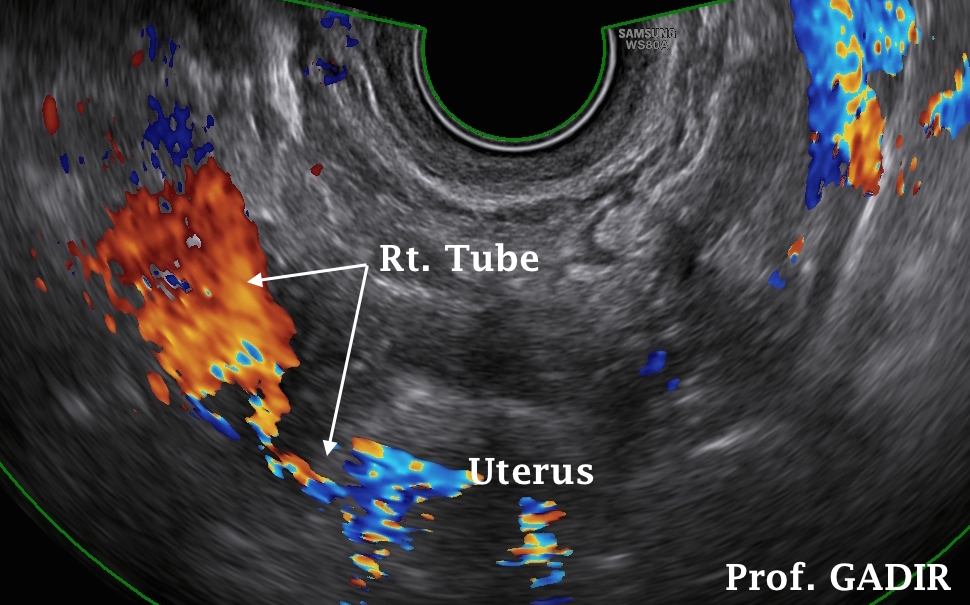
With transvaginal probe, it is easy to manipulate the uterus under vision to see each tube separately. This is not usually possible with HSG. Despite this real time advantage, it may not be possible to see both tubes together in one ultrasound plane. It needs patience and dexterity in moving the probe, as well gentle instillation of the contrast to get the best results out of HyCoSy. The two colour Doppler images shown below demonstrate better visualisation of the right and left tubes in different planes in the same patient.
HyCoSy and 3D Technology
Using 3D technology would allow storage of the volume for future examinations in different angles and planes. The 2 photographs shown above illustrate the multiplaner set of pictures used to create a 3D coronal cast view of the uterus and tubes. The ability to rotate the images in different planes could reveal any abnormal displacement of one or both tubes.
Contraindications
As for saline infusion sonohysterography, HyCoSy is contraindicated during pregnancy and in cases of suspected pelvic infection.
Methylene blue dye test
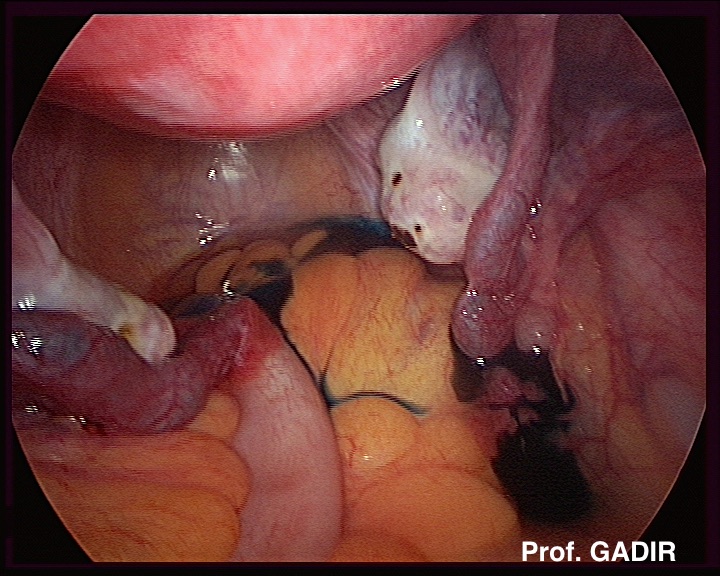
Other than HSG and HyCoSy the tubes could be tested using methylene blue dye during laparoscopy. It is a reliable procedure and other parts of the pelvis could be examined and any adhesions or endometriosis could be dealt with at the same time. However it is an invasive procedure usually done under general anaesthesia. Occasionally spasm of one or both healthy looking tubes could give a false impression of obstruction. In these cases another method of testing the tubes would be needed to verify the results. Laparoscopy is usually indicated as a primary procedure in patients with symptomatic infertility [dysmenorrhoea and deep dyspareunia], previous pelvic surgery, long history of unexplained infertility or when clinical or ultrasound examinations showed some pelvic abnormality.
The neighbouring laparoscopic photograph shows a pelvic view with patent fallopian tubes, seen hanging below the level of the ovaries. This photo is shown here to give an idea of how the pelvis looks like in real life to sonographers who are not normally involved in laparoscopic surgery.