Recurrent Miscarriages
The WHO defined a miscarriage as pregnancy loss of a fetus 500 g or less in weight. However, clinically the diagnosis relates to pregnancy loss between 5 and 20 weeks.
Sporadic loss of pregnancy is estimated to occur in 15-25% of clinically recognised pregnancies, but may exceed 50% of all conceptions. It is estimated that approximately 5% of women have 2 miscarriages, and <1% have 3 consecutive miscarriages, which is described as recurrent.
Depending on the gestational age, a miscarriage is described as early or late, if it occurred before or after 12 weeks respectively. Early miscarriages can be further sub classified into:
- Biochemical with a positive beta hCG, but no gestational sac on ultrasound scan examination.
- Anembryonic, when there is no yolk sac with a 20 mm gestation sac, and no fetal pole with a gestation sac of 25 mm or more.
- Embryonic, when there is no fetal heart activity in a 6 mm CRL fetal pole or loss of a previously observed such activity.
Causes of recurrent miscarriages
Though recurrent miscarriage is traditionally defined as 3 consecutive losses, no difference was seen in the risk of further miscarriages after 3 or 2 losses. This risk was estimated as 30-45%, or 30%, after 3 or 2 miscarriages respectively. Accordingly, patients may well be investigated after 2 losses. In all cases the rate of pregnancy loss increases with age.
There are two important points to remember when dealing with couples with recurrent miscarriages:
- Pregnancy loss is unexplainable in almost 50% of the cases, and no specific cause may be found,
- On the other hand, more than one factor may be involved in any one case, so the investigation net should be wide enough.
Almost all suspected causes can be included within two major groups:
- Problems with the pregnancy itself,
- Problems with the pregnancy environment.
Problems with the pregnancy environment
This includes a long list of factors, and transvaginal scan examination can have a major role in the diagnosis.
Anatomical factors
Cervical incompetence
Historically cervical incompetence was the most suspected anatomical cause of repeated second trimester miscarriages, though the evidence has not always been overwhelming. It is defined as inability of the cervix to support a pregnancy to term due to functional or structural defects. It is prevalent in 0.2 % of the general obstetric population, but has been described in 8% of women with history of previous midtrimester miscarriages. Animal studies documented defective tensile strength of the cervix due to rearrangement or disorganisation of the collagen fibres.
Unfortunately, there is no objective diagnostic test to be done in-between pregnancies. Clinical suspicion is most important, as hysterosalpingography and painless passage of size 8 dilator into the cervical canal are not reliable.
However, during pregnancy 3 ultrasound scan criteria are used to help with the diagnosis. Transvaginal scan examination gives better quality images than transabdominal scanning, hence it is used for that purpose. The 3 criteria used are:
- A short cervix is considered as a good primary parameter to use.
- Shortening of the cervix during repeated examinations during pregnancy can follow increased uterine muscle activity, or inherent cervical weakness.
- Dilatation of the internal cervical os, with the consequent characteristic ultrasound funnelling are important findings.
All these factors put together, may facilitate ascending bacterial infection, which can weakens the exposed prolapsed membranes. This can lead to painless spontaneous rupture of the membranes.
Uterine anomalies
Both major and minor uterine anomalies are prevalent in 7-8% of fertile women, and in more than 25% of women with recurrent miscarriages. However, major anomalies prevalence was estimated to be 3% in fertile and infertile women but 5-10% in patients with recurrent miscarriages. Uterine anomalies are related to mullerian ducts complete or partial failure of fusion or failed canalisation.
A summary of the reproductive performance of women with uterine anomalies is as follows:
- Arcuate uterus with a concave upper cavity of < 1 cm intrauterine indentation has no impact, though contradictory reports have been published suggesting more second trimester and pre term delivery with this anomaly.
- A septate uterus has 25.5 % risk of miscarriage but its impact on infertility is less known. With continued pregnancy there is increased incidence of of malpresentation and caesarean section rates. After incision of the septum there is 2-3 fold improvement in pregnancy outcome, but it does not improve pregnancy rates in infertile patients.
- A bicornuate uterus is associated with slightly increased risk of second trimester miscarriages and preterm deliveries probably due to an associated cervical incompetence. It is not recognised as a cause of first trimester pregnancy loss, and does not cause infertility. Unlike the septate version, surgical treatment is not usually indicated and can be resorted to as a final option. Follow up of the patient with serial scans for early detection of cervical incompetence and insertion of a cerclage is the first line of management. Should surgery be indicated, it should be transabdominal or laparoscopic but not hysteroscopic.
- Didelphic uterus is associated with 20% miscarriage rate and 24% preterm delivery rates.
- A unicornuate uterus has significant effect on reproduction due to abnormal uterine vasculature and decreased muscle mass. The ectopic rate is increased to 4.3%, miscarriage rate 34.4%, preterm labour 43.3% and live birth 54.2%. Moreover, there is a high caesarean section rate with this abnormality due to malpresentation and abnormal uterine contractions. It has a banana shape cavity on transvaginal ultrasound scan examination.
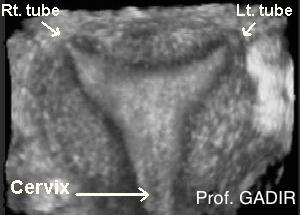
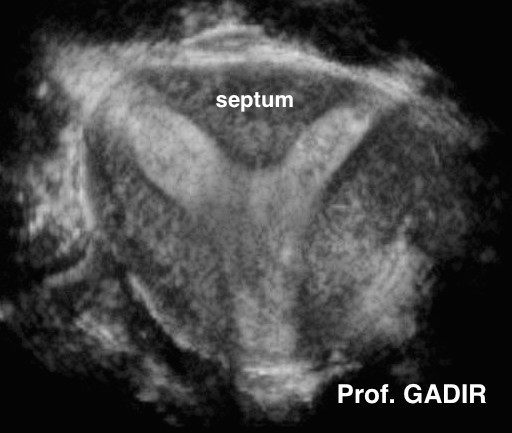
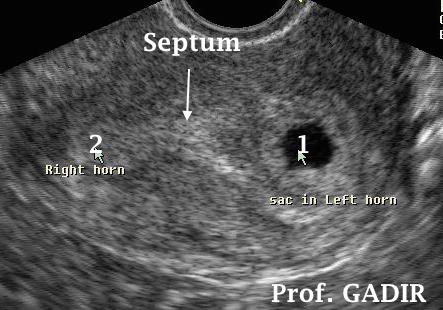
The first 3D image above shows an arcuate uterus. The second one depicts a complete septate uterus, and the third one shows a subseptate uterus. The fourth image shows a banana shaped unicornuate uterus after saline infusion hysterography.
- The first 3D image shows a pregnancy sac in the right cornual part of an arcuate uterus. This lady went on and had a term spontaneous delivery.
- The second 2D image shows an axial view of a subseptate uterus. The two horns are annotated as 1 and 2, separated by a septum covered with thick decidua. The horn marked 1 is occupied by an early pregnancy sac. She had two unsuccessful pregnancies in the past, and presented with early bleeding during the pregnancy shown above. This pregnancy ended as 14 weeks miscarriage. This was followed by hysteroscopic metroplasty, followed by successful pregnancy. Please click the link below to see how this was done using scissors.
Fibroids
The presence of submucous fibroids is widely accepted as a cause of recurrent pregnancy loss. As well, recent research showed that relatively large intramural fibroids [> 4 cm in diameter] can compromise reproductive performance. Lower implantation rate following IVF has been described in such cases, even without involvment of the uterine cavity. Research from Japan attributed this effect to lower endometrial and subendometrial blood flow, due to syphoning of the blood by the nearby fibroid.
The best way to assess how much the cavity is affected by a fibroid is through saline infusion sonohysterography, It can also show how much of the fibroid extends into the uterine muscle. This is an important information which can not be asecertained with hysteroscopy. Furthermore, saline infusion is important for deciding the best surgical approach to remove such fibroids.
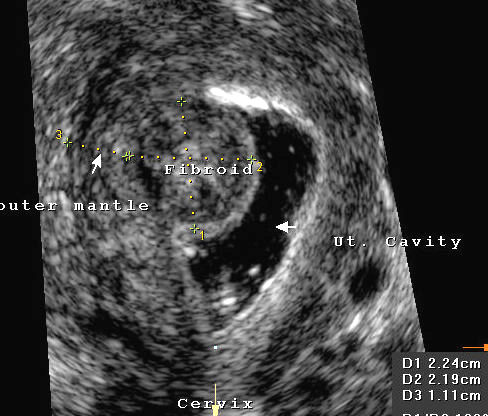
The 3D image shows grade 1 submucous fibroid, rising from the right fundal area of the cavity. Despite the small size of the fibroid, this patient had a successful pregnancy only after its excision, following two recurrent early miscarriages.
Irrespective of size, both types of fibroids are capable of causing abnormal uterine bleeding, as well as pregnancy failure. Grade 2 fibroid on the other hand is diagnosed when more than 50% of the tumour falls in the neighbouring myometrium, outside the uterine cavity.
It is important to measure the safety zone between the outer edge of the fibroid and the outer uterine serosa before attempting to remove large grade 2 fibroids. Depending on experiences 5.0 - 10 mm is the minimum safety zone required. With a smaller such zone, laparoscopy should be used, when attempting to remove such fibroids hysteroscopically.
Intrauterine adhesions
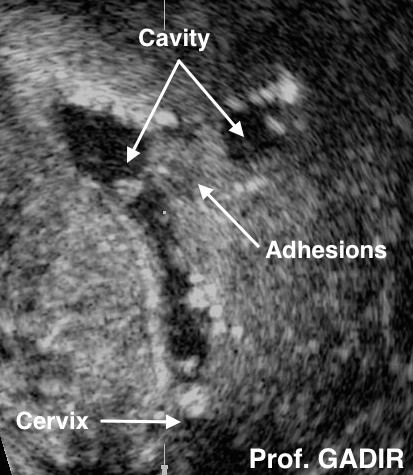
These are scar tissues which form inside the uterus as a result of infection or previous surgery. They may results from any surgery involving the uterine cavity, especially evacuation of retained products of conception. They can reduce or stop menstrual blood loss, and cause infertility or repeated miscarriages. Usually patients give history of such procedures during consultation. As well, saline infusion sonohysterography is the best method for diagnosing intrauterine adhesions. In severe cases and with apical synechiae obstructing the isthmic part, the uterine cavity usually fails to distend with the fluid.
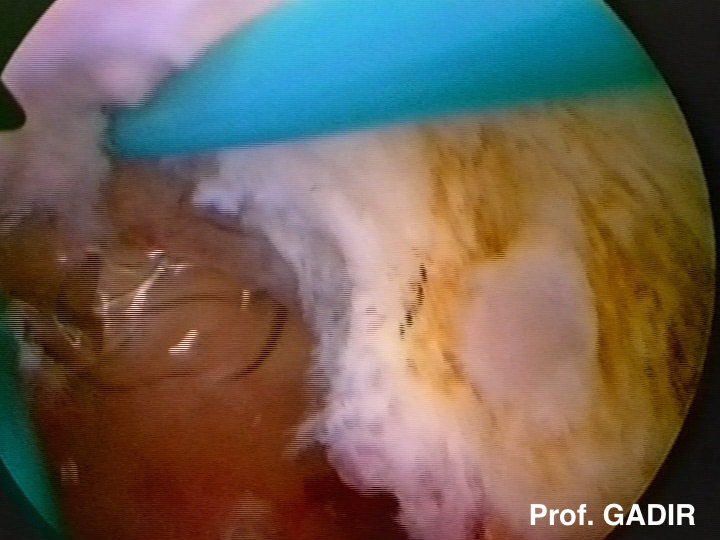
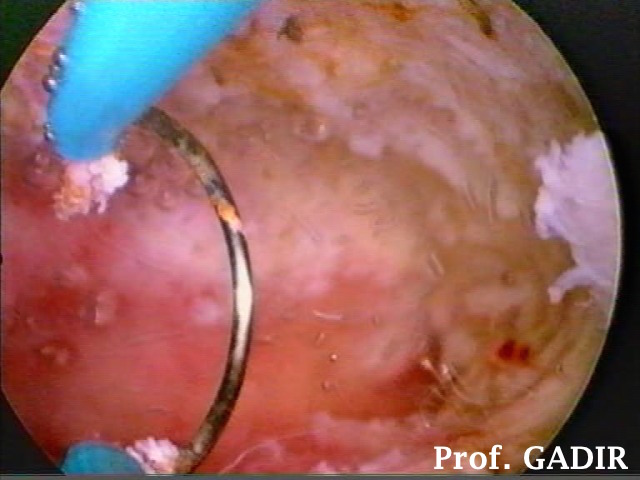
The first 3D ultrasound image shows dense intrauterine adhesions on the top and left side of the uterine cavity. This patient had open myomectomy in the past. The above 3 hysteroscopic images show few steps during the procedure for removing those adhesions, shown in the first image, using a resectoscope.
Large endometrial polyps
These are tumours of the basal endometrium with fibrous stroma and central blood vessels. According to classical teaching, large polyps can compromise early pregnancy, and need to be removed. However, there is some evidence now that irrespective of their size, polyps can interfere with embryo implantation, as shown during IVF treatment cycles. Accordingly, all polyps are currently routinely removed before any assisted reproductive treatment is offered. For more information about polyps, please have a look at the corresponding chapter in the side menu.
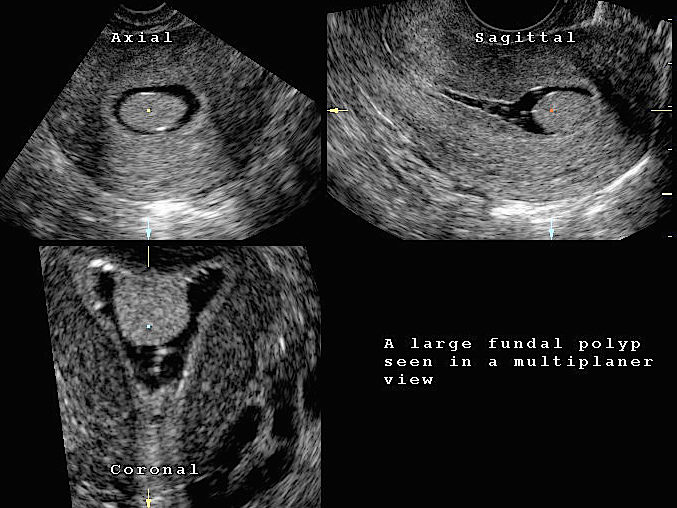
- The first multiplanar ultrasound image shown above, depicts an endometrial polyp seen in axial, sagittal and finally coronal view. Only the coronal view showed the fundal origin of the polyp, and how much of the cavity it occupied, as shown by saline infusion.
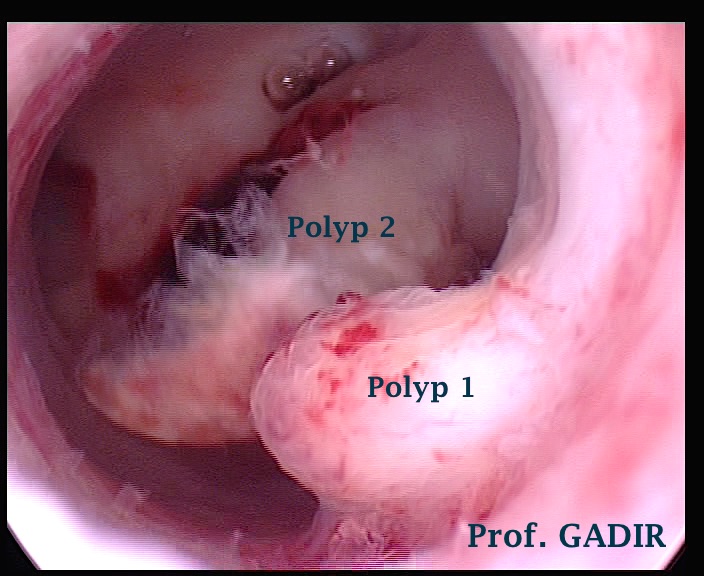
- The second image above is a hysteroscopic view of two large endometrial polyps. Without the fluid distension of the uterus during hysteroscopy, these two polyps most certainly occupied the whole cavity.
Non-anatomical factors
The following factors are not ultrasound related, but are included for the sake of completion. More information can be obtained from sites specialised in the respective fields.
These are not as common as they were thought to be few years ago. Inadequate luteal phase was thought to be an important factor but treatment with progesterone failed to show significant effect in preventing recurrent miscarriages. The same was true for repeated injections of hCG to stimulate the corpus luteum. Studying luteal serum progesterone level is not helpful in the diagnosis of management of this problem. Even endometrial bipsies which were considered to be most diagnostic of indaquate luteal phase have been shown to be unreliable. Parous women with no fertility issues were shown to have endometrial biopsies 2 or more days out of phase.
However certain endocrine problems are important in causing pregnqancy loss but they are usually clinically manifest beforehand. Thyroid problems could be related to pregnancy loss but only when the condition is very severe. The presence of thyroid antibodies without manifest hormonal defects has no bearing and the patient should not be treated accordingly.
Similarly diabetes mellitus is not a risk factor by itself unless it is not well controlled. However patients should be advised not to get pregnant unless the HBA1c level is < 7.5%.
On the other hand the increased risk of pregnancy loss with PCOS is thought to be related to high levels of insulin and androgens but not to luteinising hormone. High androgens levels have been shown to affect both oocyte quality and endometrial receptivity. Reduction of LH level by GnRH analogues did not improve miscarriage rate in women with high LH. On the other hand metformin which is a category B drug has been found to reduce the miscarriage rate in patients with PCOS and insulin resistance. Accordingly its use during the first trimester should be considered and discussed with patients with PCOS who had repeated pregnancies loss.
Immunological factors
Different immunological problems are being implicated as important causes of recurrent miscarriages and different investigations and treatment protocols are being used to address them. Two main theories have been put forward to explain how these factors could affect pregnancy outcome:
- Impairment of angiogenesis or development of blood vessels leading to occult or very early miscarriages.
- Increased clotting in preformed placental blood vessels leading to miscarriage and late pregnancy loss .
Thrombophilia with hypercoagulable conditions could be due to congenital defects in the colagulation pathway resulting in increased thrombin formation. The most common defects include mutation in factor V Leiden, a mutation that results in resistance to activated protein C which is necessary to control thrombin formation. Prothrombin gene mutation and hyperhomocysteinaemia are also common. Less frequent causes include protein S, protein C and antithrombin deficiency.
Autoantibodies to phospholipids are responible for the well known antiphosphplipid syndrome. It is associated with both early and late pregnancy loss including early miscarriages, stillbirth and neonatal death. Furthermore it has non-reproductive effects secondary to the increased coagulation tendency associated with the syndrome.
It is important not to forget the role of endometrial receptivity and blood flow in the uterine artery and subendometrium in facilitating or hindering implantation of embryos. An adverse immunological effect on the uterus could lead to a thin endometrium with low uterine and subendometrial blood flow. Recent research showed that even at 4-5 weeks gestation age uterine artery resistance index was higher in women who had recurrent miscarriages than a control group. This was suggestive of the detrimental effect of poor uterine perfusion at such an early stage.
Women with recurrent miscarriage were reported to have high peripheral and endometrial natural killer cells or activity and reduced expression of alpha-1 and -4 integrins in their blood vessels, high T-helper-1 and low T-helper-2 cytokines and reduced concentration of endometrial proteins glycodelin and MUC1. These are examples of the vast load of literature building up in this field in addition to the antiphosphplipid syndrome effect.
A personal or family history of autoimmune problems might be present including thyroid disease, rheumatoid arthritis, endometriosis or even repeated pregnancy wastage .
Life style issues
This is a vague area which is difficult to measure. However maternal smoking, use of illicit drugs and excessive alcohol intake are known to increase the risk of pregnancy loss. Few other environmental factors are incriminated with no good evidence. However tetrachloroethylene which is used in dry cleaning and accutane need special mentioning here.
Body weight extremes have also been associated with adverse pregnancy outcome. Accordingly women should be advised to follow a healthy life style with healthy dieting and excercise to attain a BMI as near to normal as possible before getting pregnant.
Pelvic infection
Few years ago pelvic infection was considered an important cause of repeated miscarriages. This view is no longer valid and routine detailed investigations for this entity are not warranted. However infection could contribute to sporadic miscarriages. This could be caused by such organisms as toxoplasmosis, bacterial vaginosis, primary infection with rubella and cytomegalovirus. On the other hand untreated endometrial ureaplasma infection could be associated with repeated miscarriages. Syphilis should not be forgotten as a cause of second trimester miscarriages in certain areas of the world.
A structured investigation programme is needed to make a diagnosis before offering any form of treatment. This would include a detailed medical history and examination. Tailored investigations would include the following:
Transvaginal scan examination and saline infusion hysterography will be necessary to exclude all the anatomical causes mentioned above. A monitored cycle with Doppler studies would help in documenting the maximum thickness of the endometrium and the echogenic pattern just before ovulation. As well Doppler studies of the uterine artery and subendometrial blood flow would give valuable information as to the perfusion of the endometrium necessary for adequate receptivity. All these tests are designed to reflect endometrial receptivity which is defined as the maturation state of the endometrium at the time of blastocyst implantation. This is a simplistic way of assessing the complex interaction between the endometrium, ovary and embryo which results in increased endometrial vascularity and oedema, enhanced glandular secretions and development of pinopodes on the luminal epithelium at the time of blastocyst implantation.
Endocrine tests would include day-3 of the cycle FSH, oestradiol and inhibin B to test for the ovarian reserve. This could be supplemented with transvaginal scan examination to measure the volume of the ovaries and to count the number of antral follicles in each ovary. Occasionally early follicular scan examination could reveal rapid recruitment of multiple follicles which is a biological evidence of incipient ovarian failure especially in women with short follicular phase. Recently anti-mullerian hormone assessment bacame available as a more reliable measure of ovarian reserve. Unlike FSH or inhibin it does not need any special timing during the cycle. Patients with very low ovarian reserve produce low quality eggs liable to pregnancy failure if fertilised and implanted. For patients with a suspected PCOS diagnosis the profile would include fasting insulin and glucose, LH, testosterone and SHBG.
Immunological tests including:
Anticardiolipin antibodies
Lupus anticoagulants
Anti beta globulin antibodies
Coagulation studies
Factor V Leiden mutation screening
Anti nuclear and antithyroid antibodies
Natural killer cells activation tests
Activated protein C resistance
Prothrombin gene defect
Hyperhomhocysteinaemia
Antithrombin III
Protein C and protein S deficiency
Total immunoglobulins
Genetic tests
Blood test for peripheral karyotyping of both partners is necessary. On the other hand testing for Y-chromosome microdeletions is indicated especially in oligoathenozoosermic men.
Routine karyotyping of products of conception is not necessary for all cases. It could be useful to allay patients anxiety if the result showed aneuploidy which would exclude a maternal cause for the problem.
Furthermore recently sperm bfragmentation test which is a measure of chromatin integrity has become available as well as sperm aneuploidy test.
Both partners should be screened for DQ alpha genes similarity.
Treatment
Treatment should target the suspected causes and followup with serial scans during the subsequent pregnancy would be essential. The most gratifying results followed removal of endometrial polyps, submucous fibroids and intrauterine adhesions. Excision of an intrauterine septum is also important to improve pregnancy outcome but the results for other uterine malformations are controversial. This mostly so for a bicornuate uterus. A successful pregnancy outcome of 76% was reported after removing intrauterine septa compared to 20% in the untreated group. Large intramural fibroids > 4 cm in diameter should be removed as well as they were shown to have an adverse pregnancy outcome. It is important to mention that insufficient data is currently available to assess pregnancy outcome following uterine artery embolisation which is gaining momentum in controlling fibroids size in recent years.
Treatment of endocrine conditions improves pregnancy outcome. Controlling insulin resistance with metformin in patients with PCOS has been shown to reduce miscarriage rate. As well a trend for lower rate of miscarriage was noted after ovarian diathermy in patients with PCOS compared to gonadotrophin treatment. Following both treatment modalities there is an expected reduction in the level of androgens which are known to affect both egg and endometrial quality. Androgens levels were shown to be negatively correlated with uterine fluid placental protein 14 [PP14 or glycodelin A] concentrations. Furthermore a higher level of free androgens was seen in women with repeated miscarriages compared to a fertile control.
Preimplantation genetic diagnosis (PGD) is potentially a good option to help with the selection of normal embryos for replacement within an assisted reproduction treatment programme for couples with repeated miscarriages due to chromosomal abnormalities. Fluorescent in situ hybridizatin (FISH) could be used to detect structural and numeric chromosomal anomalies in up to 11 chromosomes at the time being. On the other hand polymerase chain reaction (PCR) could be used to detect monogenic disorders. Ideally PGD should be offered to all women over the age of 40 years due to the increased risk of aneuploidy shown by cytogenetic tests. However there is still some controversy regarding its value in this respect. Ovum and sperm donation in licensed centres would sort this problem for those who have no religious or personal objections for this option.
Aspirin, heparin and steroids have been used singularly or in combinations to deal with recurrent miscarriages associated with thrombophilia. Aspirin which has been used to prevent thrombocytes aggregation and thromboxane release was not effective when used singularly to prevent recurrent early miscarriages. However, in combination with heparin they were shown to reduce miscarriage rate in patients with antiphospholipids syndrome and inherited thrombophilias. The recommended daily doses for aspirin and low molecular weight heparin are 75 mg and 30-40 mg respectively. However, the time when to start medication is not agreed upon. It can be started as soon as a pregnancy test is positive, though others take visible fetal heart activity after 6 weeks of pregnancy as the starting point. Patients with hyperhomocysteinamia should take vitamin B and folic acid. Other forms of immunotherapy include steroids and intravenous immunoglobulin G. The later one has not commanded universal acceptance by all specialists though good results have been reported when used for patients with high natural killer cell activity. In the last few years, intralipid 20% has replaced immunoglobulin G for the management of patients with immunologically repeated miscarriages. They were found to have similar efficacy, with the added advantage to intralipid not being a blood product, hence theoretically safer.
Important note
It is important to mention that even after 3 miscarriages there is more than 60% chance of having a successful pregnancy outcome without any treatment. Accordingly empirical treatment should be avoided. It is also important to remember that more than one factor may be involved. Furthermore, finding one abnormality does not indicate that it the definite cause of pregnancy loss. This is especially so in women with mixed obstetric history.