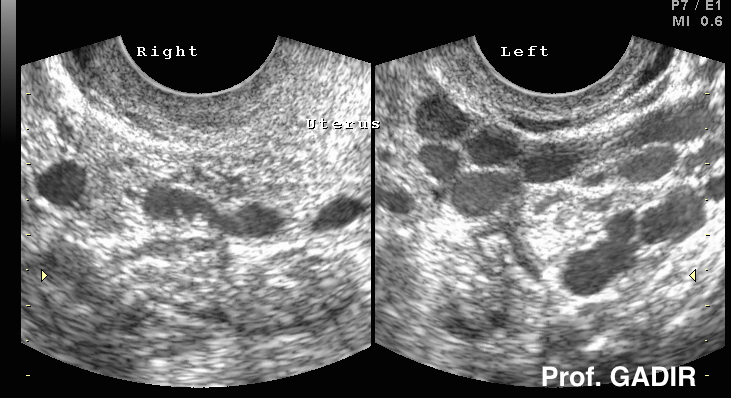
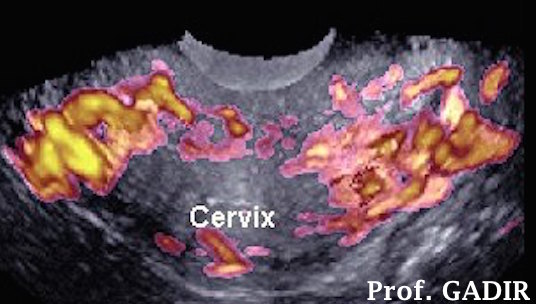
The three images shown below belong to one patient who presented with pelvic ache, persistent mucoid vaginal discharge, dysmenorrhoea and postcoital pain.
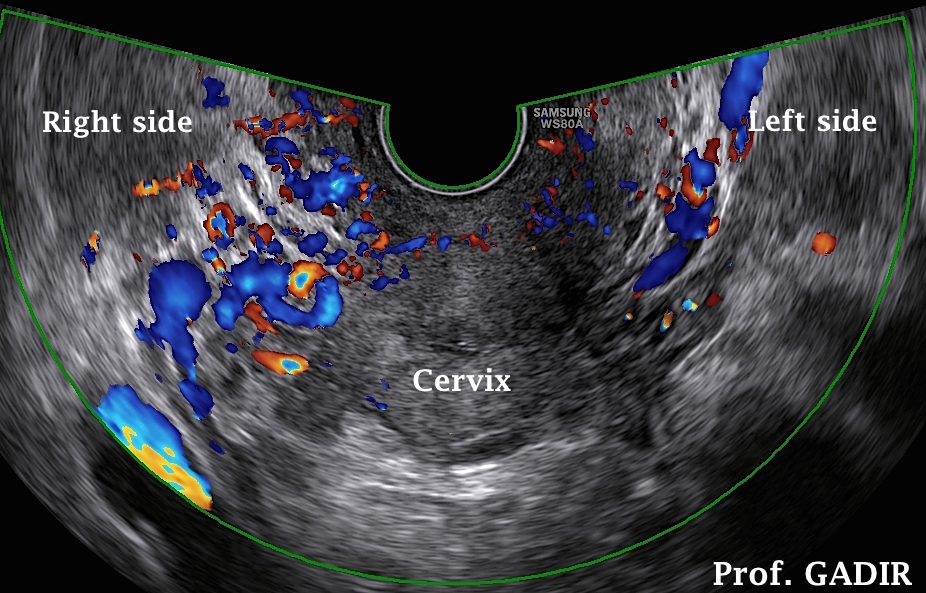
- The first colour Doppler image shows increased vascular markings on the right side of the cervix, contrary to what is usually seen in patients with pelvic congestion syndrome.
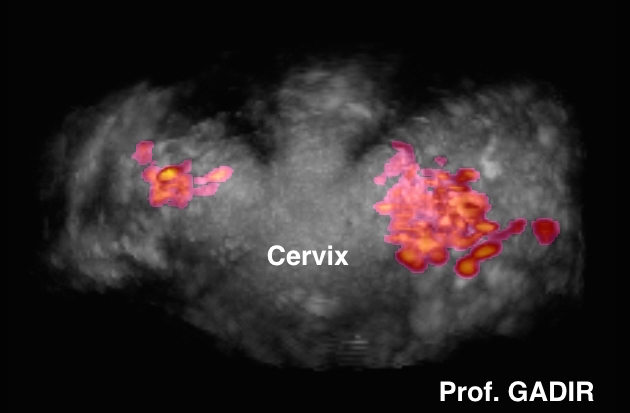
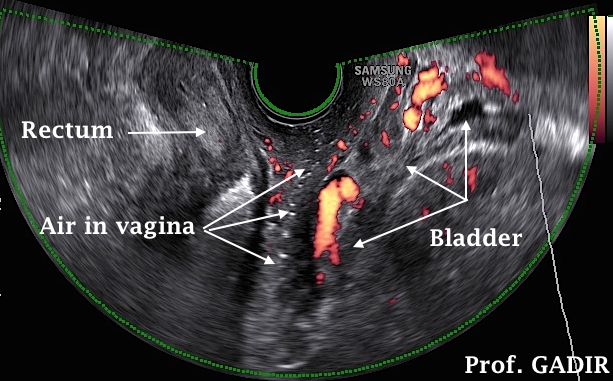
- The second power Doppler image shows very vascular area between the bladder, urethra and the vagina. This may prove to be important information when dealing with patients booked for pelvic surgery.
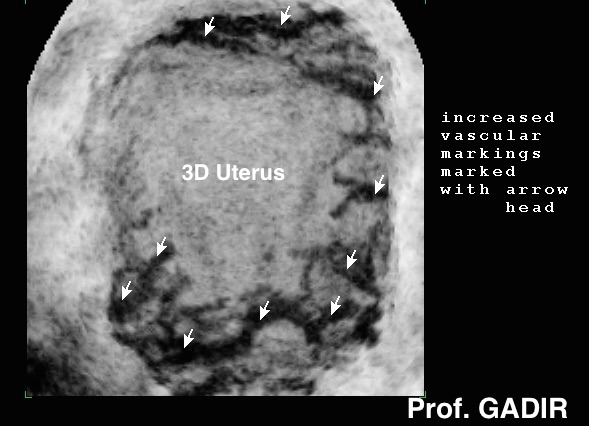
- The third power Doppler image shows very increased vascularity of the uterus reaching down to the endometrial line, despite the image being acquired immediately after menstruation.
This case demonstrated that pelvic congestion may affect all pelvic organs. Also note the very thin endometrium, despite the common observation that women with pelvic congestion syndrome usually have thick endometrium, hence their liability to abnormal uterine bleeding.
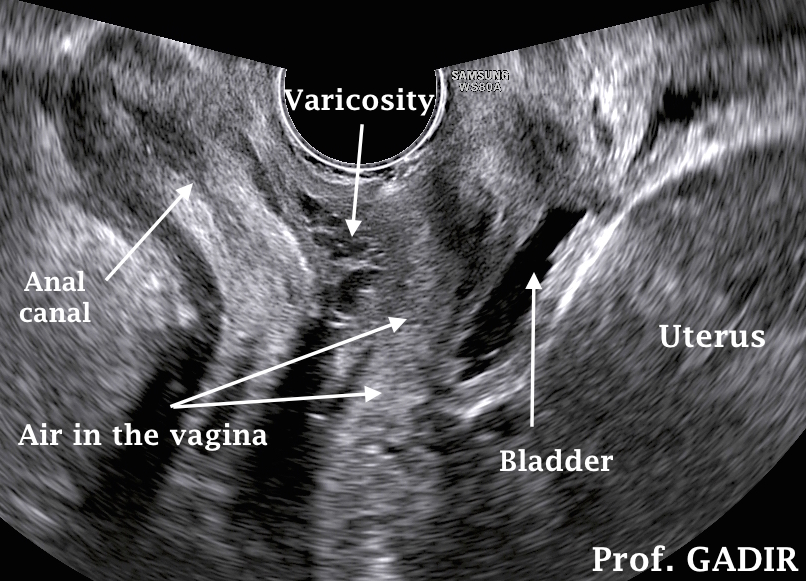
The neighbouring image, on the other hand, shows
increased vascular markings in the rectovaginal
septum [between the vagina anterioly and the rectum
posteriorly] without the need to use colour Doppler.
Opposite to the previous case, there was no increased
bladder bed vascularity. This patient presented with
vague dull perineal aching premenstrually and
increased vaginal discharge. It was not possible to
correlate the ultrasound findings and symptoms as
cause and effect. She had lower limbs varicose veins.
As mentioned before, no specific treatment has yet been agreed upon. However, both medical and surgical means have been used with variable results.
Medical treatment
Medical treatment with 30 mg medroxyprogesterone acetate (provera) every day for 6 months has been used by many gynaecologists to offer temporary relief from symptoms. In fact, reduction in the size of the dilated vessels has been demonstrated with venography after such treatment. One study showed 77% of patients treated demonstrated such an effect. Since oral contraceptive pills did not give such improvement, the effect was mostly related to the anti oestrogen effect of provera rather than actual suppression of ovulation. Unfortunately, this is a temporary remedy which lasts only while using the drug. Other treatment modalities with possible good effect include psychotherapy and using dihydroergotamine.
Surgical treatment
Surgical treatment including ovarian vein ligation, hysterectomy with and without removing the ovaries and tubes have been reported. Almost 50% of patients did not show any response after ovarian veins ligation. As well, hysterectomy did not improve symptoms, unless combined with bilateral salpingo-oophorectomy. More favourable reports followed correction of uterine retroversion and catheter embolisation of the ovarian veins, but more studies are needed to verify these results
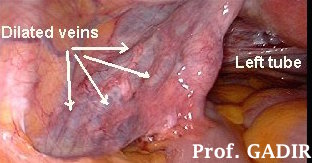
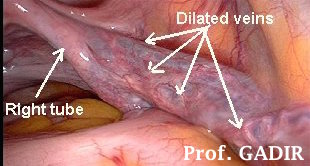
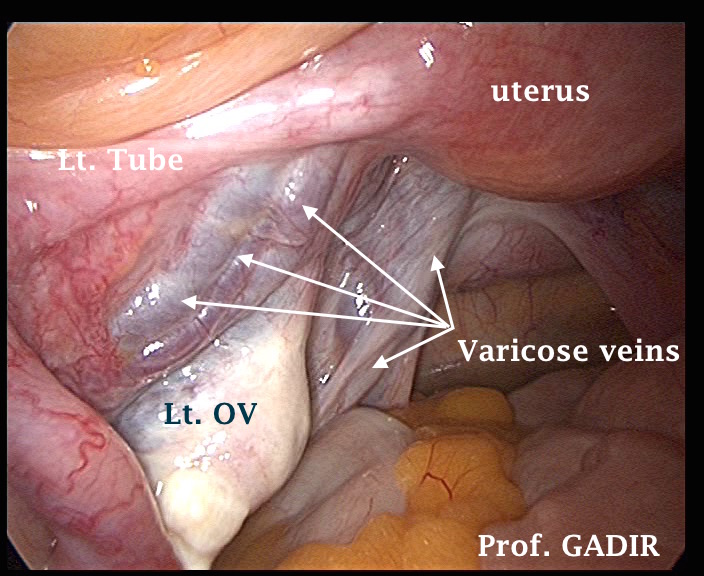
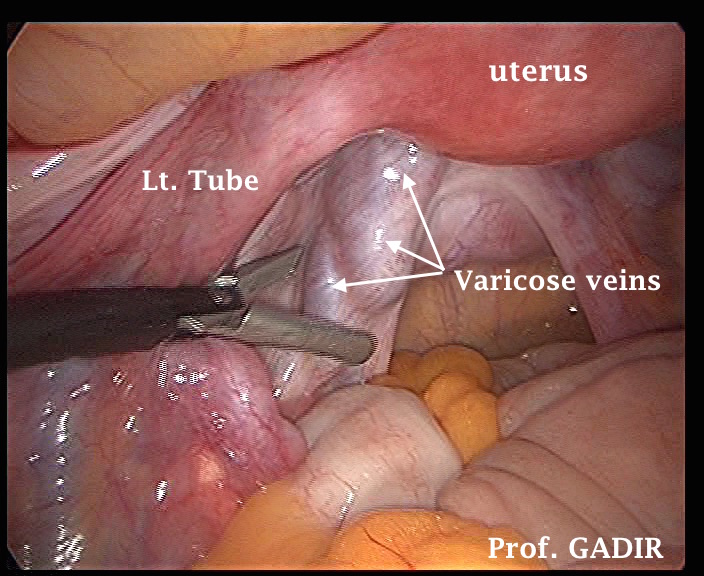
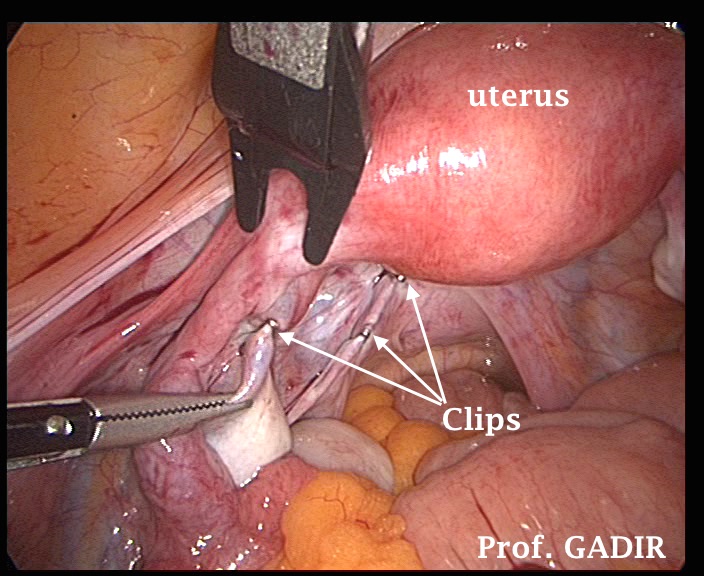
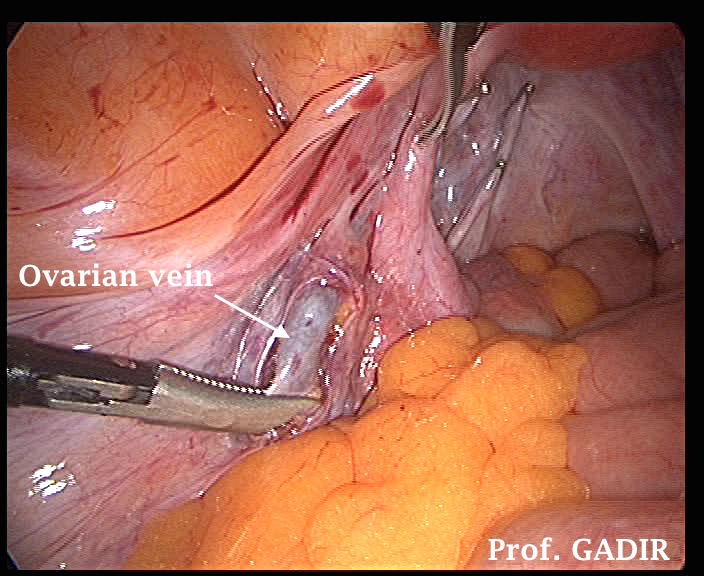
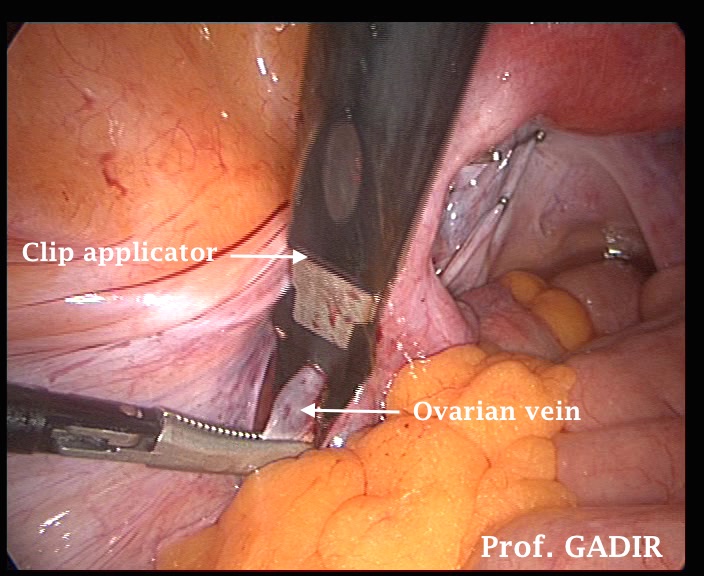
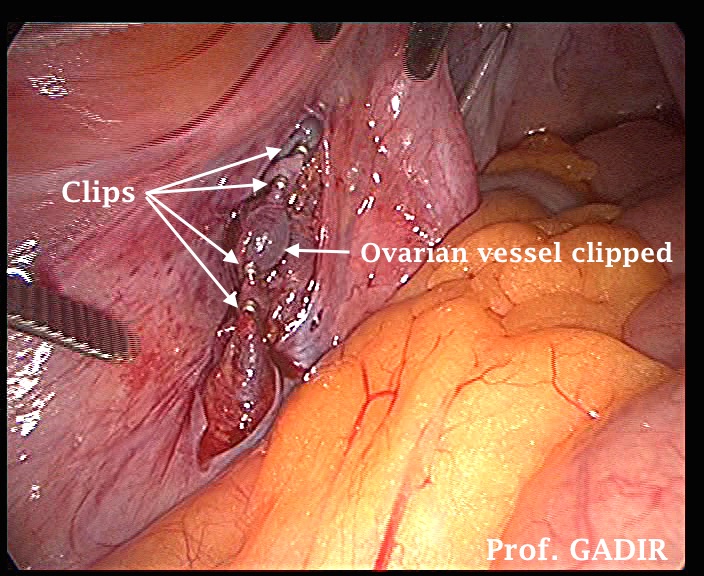
The first row of the above 6 laparoscopy shots show left pelvic sidewall varicose veins dissected and clipped. The second row show dissection and clipping of the left ovarian vein in the left infundibuloplevic ligament. Only few of the clips are shown in these shots. Varicosity can be seen lateral to the left uterosacral ligament in the pelvic sidewall, in the mesosalpinx and the left broad ligament up and lateral to the infundibulopelvic ligament. The patient had chronic pelvic pain with no other demonstrable cause. Ultrasound scan examination revealed left side pelvic congestion which did not respond to high dose of medroxyprogesterone acetate.
Important point
I saw many patients with grossly dilated pelvic veins on both sides of the uterus who had no correlated symptoms. This is a common observation in asymptomatic patients with PCOS. It may serve a big purpose to study the biodata of symptomatic and asymptomatic patients, to help with better understanding of this condition.