Ectopic pregnancy was first described in the 11th century, and since then continued to be the most frequent cause of first trimester maternal mortality. The word ectopic has been driven from the Greek word Ektopos, which means out of place. It is diagnosed when a fertilised egg implants outside the uterine cavity. Its incidence increased lately most probably because of the increased incidence of sexually transmitted diseases, especially chlamydia. 95% of all ectopic pregnancies occur along the fallopian tubes but may also occur in the ovaries, or even the cervix. The ampullary part of the tube is the most common site, but involvement of the narrow and muscular Isthmic part usually has a more dramatic effects.
Currently arround 2% of all pregnancies are ectopic, and the rate of heterotopic pregnancies also increased with the more available IVF treatment. In this case one sac will be in the uterine cavity, and the other one sited in one of the tubes, ovaries or cervix. Historically heterotopic pregnancies were quoted to occur 1 in 30000 pregnancies. However, the natural current incidence is quoted as 1 in 4000, but came down to 1 in 35 -100 with clinical pregnancies following IVF.
The first successful surgical treatment of ectopic pregnancy took place in 1759, and was performed by John Bard in New York. Since then, improvement in the managment of ectopic pregnancy improved the survival rate, despite the dramatic increase in the incidence of the condition.
In most cases development of ectopic pregnancies may not be related to any specific cause. However, certain risk factors have been identified over the years including the following:
Previous pelvic inflammatory disease which brings the issue of safe intercourse, and early diagnosis with efficient treatment of such episodes to the forefront of primary care and community gynaecology. A risk of 13%, 35% and 75% has been reported after one, two and three PID episodes respectively.
History of pelvic surgery leading to adhesions formation. Examples include appendectomy, ovarian cystectomy and myomectomy. Laparoscopic surgery is expected to cause fewer and less dens adhesions, in comparison to open surgery.
History of tubal ligation or tubal reconstructive surgery is also a risk factor. Such risk is higher 2 years after tubal ligation with electocautery due to formation of tubal / peritoneal fistulae.
Previous ectopic pregnancy increases the risk 10 times. This is mostly because the other tube might have been involved with the same pathology which contributed to the first one. Accordingly, women who conceive for the second time after an ectopic pregnancy should seek early gynaecological care for transvaginal scan examination to exclude the possibility of another one. It is important to mention that up to 15% of women who had an ectopic pregnancy in the past may have future fertility problems.
Use of an intrauterine contraceptive device, when conceived, increases the risk of ectopic pregnancy, as well. This may reach 15%, with medicated or progesterone loaded devices, compared to 5% for non-medicated devices. However, previous use of the coil does not predispose to ectopic pregnancy, unless it was complicated by clinical or subclinical pelvic infection.
Some studies related ectopic pregnancy and tubal dysfunction to smoking and regular vaginal douching. On the other hand women who conceive despite using progestogen only pills or the morning after pill are 5 and 10 times more at risk respectively.
Presentation
A high degree of suspicion should be exercised to help with diagnosing ectopic pregnancies. They are mostly diagnosed between 6-7 weeks, but may be seen at an earlier gestational age. Lower abdominal pain is the most common presentation. It can be acute in cases of ruptured ectopic with significant intra-abdominal bleeding, or subacute with or without some vaginal bleeding. With recent advances in medical care the acute presentation is not frequently seen these days. Most patients present with:
Amenorrhoea of 5-7 weeks duration.
Persistent or intermittent lower abdominal pain, which is mostly unilateral.
Abnormal uterine bleeding, which is usually mild to moderate in amount.
Positive pregnancy test, though home kits may give negative results.
Management
The main objectives in the management of patients with ectopic pregnancies are pateints' safety, high dectection rate, and avoiding the need to use laparoscopy for the sole reason of diagnosis.
In recent years more conservative approach has been adopted in treating ectopic pregnancies. Asymptomatic women, and those with a small ectopic pregnancy on ultrasound examination, and low ßhCG level, can be treated conservatively with or without intramuscular or tubal methotrexate injections. Accordingly, a good clinical assessment should be followed by blood tests for FBC and ßhCG, which should be repeated every 2 3 days. In approximately 85% of normal intrauterine pregnancies the level of ßhCG is expected to double, or at least show a 1.66 fold increase.
As well, progesterone may be a useful parameter in the management of ectopic pregnancies, as its level is constant during the first trimester. A blood level of 25 ng/ml during natural cycles is diagnostic of a normal intrauterine pregnancy, and excludes ectopic pregnancy with 97.4% certainty. However, a level < 15 ng/ml is seen in 81% of ectopic pregnancies, 93% of abnormal intrauterine pregnancies, but may as well be seen in 11% of normal intrauterine pregnancies. Because of this wide overlap, it is not a reliable diagnostic parameter in routine practice.
The role of ultrasound examination
Transvaginal scanning proved to be an important tool in the diagnosis and management of ectopic pregnancies. It may give a very high positive predictive value, and helps with the diagnosis in 90% of the cases, when performed by experienced personnel. An empty uterus with ßhCG level of 1500-2000 IU/ml may indicate an ectopic pregnancy, as at least an intrauterine sac should be seen at such levels. Alternatively, a gestational sac may be seen to the side of the uterus with or without a yolk sac, fetal pole with or without fetal heart activity. Depending on the stage at diagnosis, variable amount of fluid with floating particles can be seen in the pouch of Douglas, indicating some intra-peritoneal leak of blood from the ectopic pregnancy.
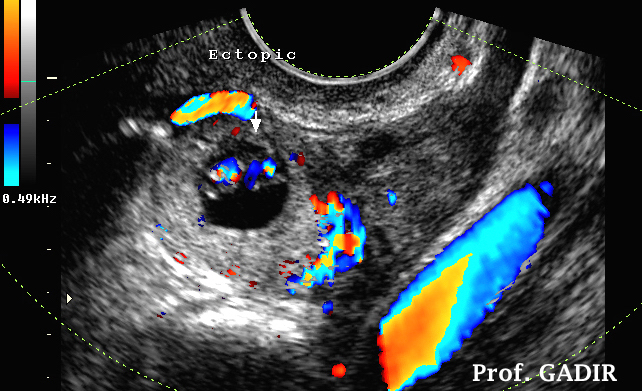
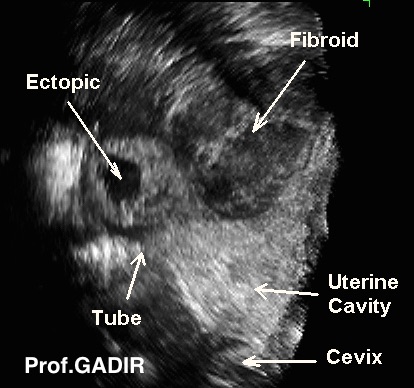
The most common ultrasound finding, in almost 80%, of the cases is the presence of a mass 'in the ectopic angle', between the uterus and the ovary harbouring the corpus luteum. However, viable ones with fetal heart activity are the least common type.
The neighbouring colour Doppler image shows an ectopic pregnancy with partial vascular ring and fetal pole showing colour markings of fetal heart activity. This is one of the least commonly seen types of ectopic pregnancy.
The presence of turbid fluid in the pouch of Douglas is an important, but not a universal finding in all ectopic pregnancies. The amount of fluid usually reflects how much blood has leaked through the fimbrial end of the tube. Major haemoperitoneum can be seen in complicated or ruptured ectopic pregnancies. With a positive pregnancy test and an empty uterus, the presence of intraperitoneal fluid is almost 70% sensitive in diagnosing an ectopic. This sensitivity may rise up to > 90% if the fluid was echogenic.
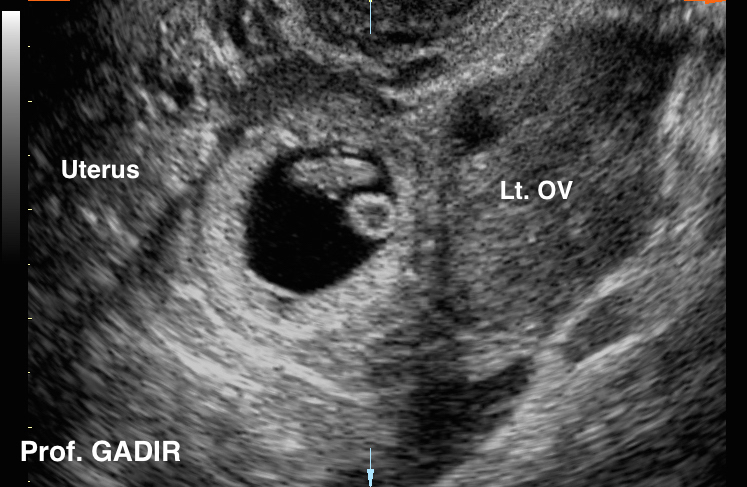
The first image above shows an ectopic pregnancy sac with a clear fetal pole and yolk sac in the ectopic angle between the uterus and left ovary.
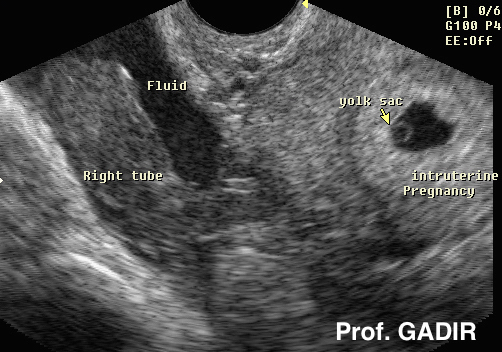
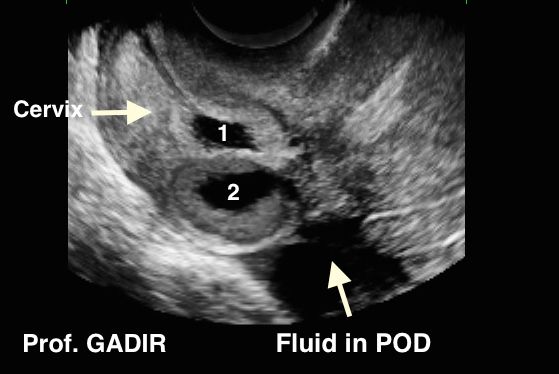
The second image shows a heterotopic pregnancy with one sac in the uterus and the other one in the dilated right tube.
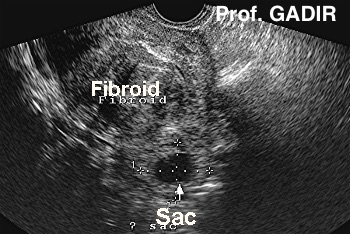
The third image shows a heterotopic pregnancy with one intrauterine and one cornual or interstitial in location.
Both heterotopic pregnancies shown above followed IVF treatment. Note the echogenic band joining the two gestational sacs in the third image. It may be much thinner than what is shown in this picture in case of a cornual pregnancy, without a concomitant intrauterine one. Such thin echogenic line extending into the cornual region, and merging with the gestational sac is known as the interstitial line, and has been found to be highly specific for interstitial pregnancies Also a cornual sac is usually surrounded by a thin layer of myometrium. Both of these characteristics are best seen in rendered coronal views after capturing a 3D volume. The presence of fluid collection or pseudosac in the uterine cavity may be seen with tubal pregnancies, and should not be confused with intrauterine gestation. A pseudosac is usually seen within the cavity, rather than towards one side or the other of the central uterine echo, which is characteristic of normal ones. Furthermore, it will not show a yolk sac or fetal pole.
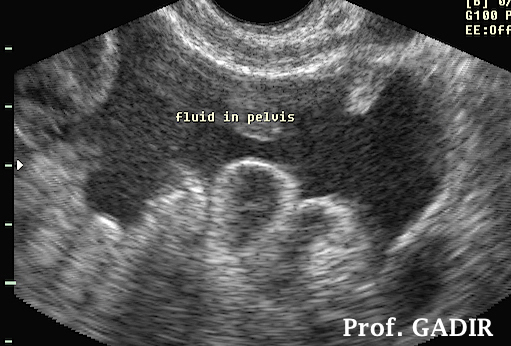
The first image above shows a pseudo sac inside the uterine cavity near the top, rather than embedded into one or another wall. Also there is no fetal pole or yolk sac. Note the presence of blood clots beside the sac in the uterine cavity. Another characteristic of a pseudo sac is the absence of any vascular markings during colour Doppler mapping. With such ultrasound finding in a patient with positive pregnancy test and turbid fluid in the pouch of Douglas as shown by the second image above, an ectopic pregnancy must be diagnosed.
Twin ectopic pregnancies
Other than the heterotopic pregnancies alluded to before, twin ectopic pregnancies can occur in the same tube, or in the cervical canal as shown by the two images below respectively. The two patients attended our clinic with abnormal uterine bleeding and positive pregnancy tests. The first one had induction of ovulation with clomiphene citrate .The second one had conceived after IVF treatment. She gave prior history of hysteroscopic surgery for intrauterine adhesions, which was complicated with perforation of the posterior cervical wall. Both patients were treated with methotrexate.
Failure to see a gestational sac within the uterus, or in one tube or the other with a positive ßhCG blood test does not rule out the presence of a pregnacny somewhere in the pelvis. This is now given the term Pregnancy of Unknown Location [PUL].
Patients with unstable cardiovascular system and those with acute onset of pain are better treated surgically. As well, a patient with a large ectopic pregnancy and identifiable fetal heart activity should be treated surgically.
Laparoscopy has already taken over as the standard method for treating ectopic pregnancies needing surgical intervention. Patients usually go home on the same day, or at most the following morning after the procedure. The tube can be easily excised and removed in a retrieval bag as shown below. This is especially done when:
There is significant haemorrhage,
The tube has ruptured,
The tube is a site of previous ectopic pregnancy,
The tube is significantly distorted,
Future fertility is not an issue.
However, in certain cases the tube may be slit on top of the ectopic pregnancy which can be removed without damaging the whole tube (salpingostomy). In such cases, there is 5-10% risk of persistent ectopic with viable chorionic villi continuing to grow. The ßhCG level will stay high, and patients may become symptomatic again within 10 days after surgery. This may lead to subsequent rupture of the tube, unless treatment with methotrexate is given or salpingectomy is performed.
Please click on the following link to see an ectopic pregnancy being removed laparoscopically:
Methotrexate is an anti metabolite which is usually used for treating some forms of cancer. It inhibits rapidly growing cells, hence used to block the growth of ectopic trophoblasts. It is usually used for small ectopic pregnancies less than 3-4 cm in diameter, in haemodynamically stable patients who have no significant intra-abdominal haemorrhage. Depending on the selection criteria more than 70% of medically treated ectopic pregnancies resolve, with confirmed tubal patency in 70% of the cases. Furthermore, they have a similar recurrence of ectopic pregnancies as compared to conservative surgery. The usual dose is 50 mg per square metre intramuscularly, though direct injection into the ectopic site is used frequently. Strict follow up of these patients is necessary for a long time till the ßhCG level returns back to the non pregnant level. However, there might be an initial transient rise in the level of ßhCG, as well as lower abdominal pain. Furthermore, it is also important to note that a mass may be seen at the ectopic site with transvaginal scanning for many months following medical treatment.
Role 3D Ultrasonography
No specific role for 3D ultrasound examinations has been established. Having said that, it is very useful to specify the exact location of the ectopic pregnancy before surgery, in difficult cases. This is especially so in cases where the uterus is distorted by multiple or large fibroids.
The two images shown above represent 2D and 3D images of the same ectopic pregnancy. It was very difficult to localise the exact location of the ectopic sac because of the presence of the fibroid. The 3D view was very helpful in this respect. The ectopic sac sat on top of the right fallopian tube in an area proved to be adenomyotic in nature after histological examination. The right tube itself was not affected. We published this case in Gynaecological Surgery [Gynecol Surg,2009 (6):267271].